HORMONES 2005, 4(2):96-100
DOI: 10.14310/horm.2002.——
Address correspondence and requests for reprints to:
Ioannis Ilias, Department of Pharmacology, Medical School, University of Patras, Rion-Patras, 26504, Greece, Phone: + 30 6932 587674, + 30 2610 997638, Fax: + 30 2610 994720, e-mail: iliasi@upatras.gr
Received 11-02-04, Revised 20-03-05, Accepted 25-03-05
Abstract
The standard intravenous short Synacthen® test (SSST) has long been accepted as one of the most reliable diagnostic tests of adrenocortical insufficiency. Intramuscular (i.m.) administration of ACTH obviates the need of venous cannulation and can be used as an alternative to the intravenous test. Nevertheless, reports of correlation between cortisol response to i.m. ACTH1-24 and 24-hr average cortisol concentration are scarce. We studied this relation in 64 nonobese healthy men. Blood samples for serial cortisol measurements were collected hourly over 24 hrs. The following day, blood samples were collected at baseline and at 30 and 60 min after intramuscular (IM) administration of 250 µg of ACTH1-24. All healthy men reached 24-hr serum cortisol peak values (Cmax) between 0600h and 1000h. Following i.m. ACTH1-24, cortisol levels significantly increased at both 30 (C30ACTH) and 60 (C60ACTH) minutes, when compared to baseline values. C30ACTH and C60ACTH significantly correlated with Cmax and with the 24-hr time-integrated cortisol concentration (AUC0-24). Morning mean cortisol was calculated as the average of serum concentrations measured between 0600h and 1000h (Cav6-10) and correlated very well with AUC0-24. In conclusion, we comfirmed that i.m. administration of ACTH1-24, followed by a single blood sampling at 60 min for cortisol measurement represents a valid, convenient and cost- effective screening test of adrenal function.
Key words: Adrenocorticotropin, Cortisol, Diagnostic use, Intramuscular injection
INTRODUCTION
Several tests are currently available to assess the integrity of the hypothalamic-pituitary-adrenal (HPA) axis. However, the reliability and accuracy of such tests in case of suspected adrenal insufficiency remains a matter of debate. Because of the circadian rhythmicity and pulsatility of cortisol concentration, a single determination of serum levels of this hormone at 0800h reflects the HPA axis activity in a representative, albeit gross fashion, since it does not provide reliable information on adrenocortical function during the rest of the day1-5. On the other hand, 24-hr serum cortisol, which overcomes this limitation, has the inconvenience of requiring overnight hospitalization6. The cortisol response to insulin-induced hypoglycemia is one of the most valuable tests of adrenal function; yet, it is cumbersome, unpleasant and potentially dangerous7.
The standard short Synacthen® test (SSST) is peformed by administering 250 µg/1.73 m2 body surface area of synthetic adrenocorticotropic hormone (ACTH1-24) intravenously (i.v.) or intramuscularly (i.m.). Both tests have long been accepted as reliable screening procedures in patients with a compromised adrenocortical reserve8-12. When performed in patients with adrenal insufficiency at any time of the day, the SSST can be diagnostic13,14. A normal response to SSST is defined as a peak serum cortisol of ≥440 or ≥500 nmol/L after i.m or i.v. ACTH1-24 administration, respectively1,15-19. However, normal subjects show a ten-fold difference in 24-hr urinary free cortisol measurments pre- and post-Synachten®20. This finding, as well as actual measurements of ACTH1-24 concentrations, indicates that a Synacthen® dose of 250 µg is pharmacologic. Thus, we sought to study the quantitative concordance between serial serum cortisol measurements and SSST in healthy subjects.
SUBJECTS AND METHODS
Subjects
Sixty four nonobese healthy men (mean ± SD; age: 24±5.4 yrs; BMI: 22.6±2.3 kg/m2) were included in the study. The subjects belonged to the placebo group of a study on the effect of budesonide and other inhaled corticosteroids on the HPA axis conducted by Schering-Plough in the Netherlands. Patients who had history of major physical or psychiatric illness, food or drug allergy, smoking or alcohol abuse, or tested positive for hepatitis B, C or HIV were excluded from the study. None of the enrolled subjects had clinical or biochemical evidence of hepatic and renal disease, or had been taking any drug known to alter cortisol binding globulin (CBG) concentrations or induce hepatic enzymes for at least one month prior to the study. The study was approved by the Medical Ethics Committee of the “Stichting Beoordeling Ethiek Bio-Medisch Onderzoek”, Assen, The Netherlands.
Methods
Patients were admitted to the hospital two days prior to the study and standard anthropometric measurements were obtained by a single trained observer. An indwelling venous catheter was inserted at least 12 hours before sampling. Patients were permitted normal ambulatory activity, but strenuous physical exercise was avoided. Standard hospital meals were given at 0800h, 1230h and 1730h.
On the first day of the study, baseline investigations were performed at 0800h, and blood samples for measurements of serum cortisol were collected hourly over 24 hours. The night before the SSST, all subjects remained supine from midnight to 0700h. On the second day of the study, 250 µg of ACTH1-24 were injected i.m. at 1100h, and blood was obtained at baseline and at 30 and 60 minutes after ACTH1-24 administration. Plasma was separated by centrifugation immediately after blood collection and stored at _20° C until assayed.
Cortisol assay
Serum total cortisol was measured using the Coat-A-Count radioimmunoassay (Diagnostic Products Corporation, Los Angeles, CA, USA). This is a solid phase assay with a sensitivity of 5.5 (nmol/L). The intra-assay coefficients of variation (CVs) were 5.7% and 2.6% at serum concentrations of 28.0 and 550.0 (nmol/L), respectively. The inter-assay CVs were 6.3% and 4.5% at serum concentrations of 140.0 and 275.0 (nmol/L), respectively.
Data analyses
Non-normally distributed data were logarithmically transformed prior to statistical analysis. Time-integrated cortisol concentration was calculated as the area under the curve of serum concentrations over 24 hours (AUC0-24), using the trapezoid method. Cortisol peak was calculated as the highest serum concentration measured in 24 hours (Cmax). Morning mean cortisol was calculated as the average of serum concentrations measured between 600h and 1000h (Cav6-10).
One-way analysis of variance (ANOVA) with the Student-Newman-Keuls (SNK) post hoc correction was used to compare cortisol responses to ACTH1-24 at 30 (C30ACTH) and 60 (C60ACTH) min vs. baseline values. Correlations between Cmax or AUC0-24 and C30ACTH or C60ACTH were tested by linear regression and calculation of Pearson’s correlation coefficient. All reported values are expressed as mean ± SD, unless otherwise specified. Statistical differences are denoted by a Bonferroni-corrected P value of < 0.05.
RESULTS
All subjects reached 24-hr cortisol peak values (Cmax, 427.6 ± 60.7 nmol/L) between 0600h and 1000h. Cmax was attained between 0800h and 0900h in 58 subjects (90.7%).
C30ACTH and C60ACTH were both significantly increased when compared to baseline values (515.9 ± 66.2 and 584.9 ± 69.0 vs. 242.8 ± 85.5 nmol/L, respectively, P< 0.001). Peak cortisol responses to ACTH1-24 were observed at 60 minutes in 61 subjects (95.3%) and at 30 min in the remaining 3 (4.7%). All the subjects achieved a peak cortisol response of ≥440( nmol/L).
Both C30ACTH and C60ACTH showed correlation with Cmax (r = 0.454 and 0.459 respectively, P< 0.001) (Figure 1, A and B) and AUC0-24 (r = 0.549and 0.537, respectively, P< 0.001) (Figure 1, C and D). Additionally, we found positive correlations between Cav6-10 and AUC0-24 (r = 0.709, P<0.0001) (Figure 2A), C30ACTH (r = 0.249, P <0.05) (Figure 2B) andC60ACTH (r = 0.226, P= 0.07) (Figure 2C).
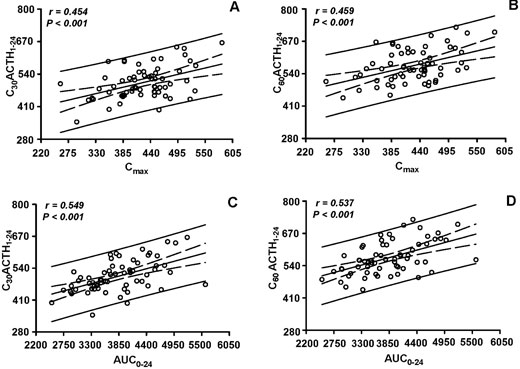
Figure 1. Scatterplots of cortisol responses to i.m. ACTH1-24 at 30 (C30 ACTH1-24) and 60 (C60 ACTH1-24) min vs. 24-hr serum cortisol peak (Cmax) (A and B, respectively) and 24-hr time-integrated cortisol concentration (AUC0-24) (C and D, respectively). Regression lines are shown with their 95% confidence intervals. Cortisol concentrations are in nmol/L, AUC are in nmol/L x h
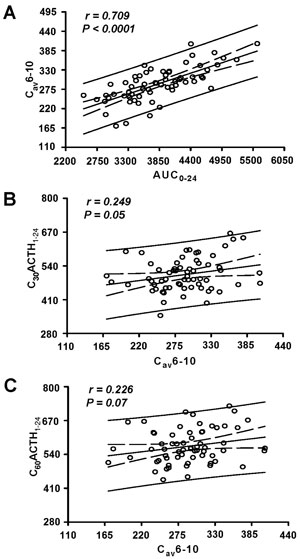
Figure 2. Scatterplots of morning serum cortisol average between 0600h and 1000h (Cav6-10) vs. AUC0-24 (A), C30 ACTH1-24 (B) and C60 ACTH1-24 (C). Regression lines are shown with their 95% confidence intervals. Cortisol concentrations are in nmol/L, AUC are in nmol/L x h.
DISCUSSION
Several medical conditions can alter adrenocortical homeostasis causing abnormal adrenal function. Chronic glucocorticoid treatment, infections, autoimmune adrenalitis, infiltrative or neoplastic diseases, as well as congenital or acquired abnormalities of the HPA axis are among the most common causes of adrenal insufficiency11. Unfortunately, many symptoms related to adrenal failure, such as weight loss, anorexia and fatigue are nonspecific.
Many laboratory tests are currently available to assess the integrity of the HPA axis, each one with its own advantages and limitations1-5. The use of synthetic ACTH1-24 given i.v. or i.m. at low or high dose (500 ng or 250 µg/1.73 m2 body surface area, respectively) are among the most frequently used test in clinical practice. The low-dose ACTH test, which may offer high reliability in the diagnosis of mild forms of primary hypoadrenalism, is less sensitive in the diagnosis of secondary hypoadrenalism21. Serial measurements of serum cortisol levels over 24 hours provide accurate information about the functional status of the HPA axis, given the ability to reveal pitfalls in the pulsatility and circadian rhythm of cortisol concentration6. However, they are costly and often subject to low compliance from the patient.
Cortisol values of ≥ 440 (nmol/L) in response to i.m. ACTH1-24 were detected in all of our study subjects. The large majority reached a cortisol peak response at 60 min, suggesting that blood sampling at 30 min may be unnecessary during i.m. SSST.
These findings, while confirming our previous observations16, strongly support prior reports of similar cortisol responses with similar cut-off values after i.m. and i.v. ACTH1-24 administration1,19,22. Furthermore, we showed for the first time that cortisol responses to i.m. ACTH1-24 correlates with 24-hr cortisol serum peak (Cmax) and time-integrated concentration (AUC0-24), which are both reliable indices of HPA axis endogenous activity. Interestingly, we found that morning serum cortisol average between 0600h and 1000h (Cav6-10) correlates well with AUC0-24.
Among the limitations of this study, we have to point out that we did not study patients with adrenal disease, but rather attempted to define normal relations between SSST and serial serum cortisol measurements. Another caveat is that we did not compare SSST against the gold standard insulin tolerance test for (ITT) for cortisol.
In conclusion, our results show that i.m. administration of ACTH1-24, followed by a single cortisol measurement at 60 min, is comparable to 24hour cortisol sampling and represents a valid and rapid screening test of adrenal function in healthy men. In combination with this test, the Cav6-10 may be a more reliable index of cortisol morning peak than the single morning measurement of plasma cortisol. Further validation of these results in patients with adrenal insufficiency is warranted.
REFERENCES
1. Miller WL, Chrousos GP 2001 The adrenal cortex. In: Frohman LA (ed) Endocrinology and Metabolism New York: McGraw Hill.
2. Hagg E, Asplund K, Lithner F, 1987 Value of basal plasma cortisol assays in the assessment of pituitary-adrenal insufficiency. Clin Endocrinol 26: 221-226.
3. Jones SL, Trainer PJ, Perry L, Wass JA, Bessser GM, Grossman A, 1994 An audit of the insulin tolerance test in adult subjects in an acute investigation unit over one year. Clin Endocrinol 41: 123-128.
4. Pavord SR, Girach A, Price DE, Absalom SR, Falconer-Smith J, Howlett TA, 1992 A retrospective audit of the combined pituitary function test, using the insulin stress test, TRH and GnRH in a district laboratory. Clin Endocrinol 36: 135-139.
5. Watts NB, Tindall GT, 1988 Rapid assessment of corticotropin reserve after pituitary surgery. JAMA 259: 708-711.
6. Van Cauter E 1989 Endocrine rhythms. In: Waterhouse JM (ed) Biological rhythms in clinical practice, London: Wright.
7. Shah A, Stanhope R, Matthew D, 1992 Hazards of pharmacological tests of growth hormone secretion in childhood. Br Med J 304: 173-174.
8. Stewart PM, Corrie J, Seckl JR, Edwards CR, Padfield PL, 1988 A rational approach for assessing the hypothalamo-pituitary-adrenal axis. Lancet 1: 1208-1210.
9. Bangar V, Clayton RN, 1998 How reliable is the short synacthen test for the investigation of the hypothalamic-pituitary-adrenal axis? Eur J Endocrinol 139: 580-583.
10. Gleeson HK, Walker BR, Seckl JR, Padfield PL, 2003 Ten years on: Safety of short synacthen tests in assessing adrenocorticotropin deficiency in clinical practice. J Clin Endocrinol Metab 88: 2106-2111.
11. Streeten DH, Anderson GHJ, Dalakos TG, et al, 1984 Normal and abnormal function of the hypothalamic-pituitary-adrenocortical system in man. Endocr Rev 5: 371-394.
12. Laue L, Peck GL, Loriaux DL, Gallucci W, Chrousos GP, 1991 Adrenal androgen secretion in postadolescent acne: increased adrenocortical function without hypersensitivity to adrenocorticotropin. J Clin Endocrinol Metab 73: 380-384.
13. Greig WR, Browining MC, Boyle JA, Maxwell JD, 1966 Effect of the synthetic polypeptide beta-1-24 (synacthen) on adrenocortical function. J Endocrinol 34: 411-412.
14. McGill PE, Greig WR, Browining MC, Boyle JA, 1967 Plasma cortisol response to synacthen (beta-1-24 Ciba) at different times of the day in patients with rheumatic diseases. Ann Rheum Dis 26: 123-126.
15. Amsterdam JD, Winokur A, Abelman E, Lucki I, Rickels K, 1983 Cosyntropin (ACTH alpha 1-24) stimulation test in depressed patients and healthy subjects. Am J Psychiatry 140: 907-909.
16. Longui CA, Vottero A, Harris AG, Crousos GP, 1998 Plasma Cortisol responses after intramuscular Corticotropin 1-24 in healthy men. Metabolism 47: 1419-1422.
17. Faical S, Kater CE, 1991 Padronizacao e aplicacao dos testes rapido e prolongado de estimulo com ACTH em pacientes com insuficiencia adrenocortical primaria e secundaria. AMB Rev Assoc Med Bras 37: 132-138.
18. Grunwald K, Rabe T, Urbancsek J, Runnebaum B, Vecsei P, 1990 Normal values for a short-time ACTH intravenous and intramuscular stimulation test in women in the reproductive age. Gynecol Endocrinol 4: 287-306.
19. Grinspoon SK, Biller BM, 1994 Laboratory assessment of adrenal insufficiency. J Clin Endocrinol Metab 79: 923-931.
20. Sapin R, Schlienger JL, Gasser F, Pradignac A, Grucker D, 1998 Improved specificity of a new direct assay for urinary cortisol: application in corticoid-treated patients. Clin Chem Lab Med 36: 855-858.
21. Agwu JC, Spoudeas H, Hindmarsh PC, Pringle PJ, Brook CG, 1999 Tests of adrenal insufficiency. Arch Dis Child 80: 330-333.
22. Stewart PM 2003 The adrenal cortex and endocrine hypertension. In: Polonsky KS (ed) Williams Textbook of Endocrinology, Saunders Publications, Philadelphia.