Abstract
Objective: Childhood obesity is associated with impaired endothelial function, insulin resistance and inflammation. Being at risk for overweight has been defined as having a body mass index (BMI) between the 85th and 94th percentile for age and sex. In this study, we looked for features linked to cardiovascular risk in children who are at risk for overweight. Design: Twenty-one children who were at risk for overweight (study group) and 20 children with a BMI between the 25th-74th percentiles (controls) were studied. Fasting blood levels of glucose, insulin, total cholesterol, HDL cholesterol, triglycerides, uric acid, fibrinogen and high sensitive C-reactive protein (CRP) were assessed in both groups. LDL-cholesterol, HOMA-IR and QUICKI indices were calculated. Flow-mediated Vasodilatation (FMD) was determined for the evaluation of endothelial function. Results: Increased HOMA-IR was observed in children who were at risk for overweight. Waist circumference was the main predictor of insulin resistance in these children. Higher levels of CRP were found in the study group compared to controls, while plasma fibrinogen did not differ in the two groups. The children who were at risk for overweight had lower FMD values and slightly elevated lipids compared to controls; however, these differences were not statistically significant. Conclusion: Insulin resistance and inflammation indices were higher in children who were at risk for overweight as has been shown for obese children. The data suggest that appropriate treatment strategies for weight control are essential not only for obese children but also for those at risk for overweight.
INTRODUCTION
Childhood obesity has become a public health problem in developed countries, while its prevalence also shows an increasing trend in developing countries like Turkey.1 Obesity is associated with an increased risk for cardiovascular disease and mortality in adults. Insulin resistance, the main characteristic of the metabolic syndrome, can also be observed in children with obesity. Childhood obesity frequently persists into adulthood. In addition, the risk for developing metabolic syndrome and Type-2 Diabetes Mellitus (T2DM) in adulthood is increased in obese children.2
Body Mass Index (BMI) is commonly used to determine childhood overweight and obesity since it is an easy and reliable method. The use of BMI percentile for age and sex is the best method for detecting children with overweight as well as those at risk for overweight.3 According to the guidelines of the Center for Disease Control and Prevention,4 overweight is defined as having a BMI at or above the 95th percentile for age and sex, while being at risk for overweight is defined as having a BMI between the 85th and 94th percentile for age and sex. Recently, Bundak et al5 have constructed the body mass index reference curves for Turkish children, aged 6 to 18 years.
Maintaining a body weight appropriate for height is critical for the prevention of atherosclerotic disease as well as being a cost-effective strategy.6 There is evidence of a relationship between childhood obesity and early development of atherosclerosis.7-9 The Bogalusa Heart Study has shown that the 99th percentile of BMI for age confers a very high risk of development of biochemical abnormalities associated with atherosclerosis.7 Several studies have demonstrated the association of indices of acute phase reaction, endothelial dysfunction and insulin resistance (pro-atherogenic factors) with accelerated atherosclerosis in childhood obesity.8-10
Atherosclerosis is an inflammatory process that is initiated by endothelial activation.11 Endothelial dysfunction, which can be evaluated by non-invasive, flow-mediated vasodilatation (FMD), is present in obese children and is mainly associated with insulin resistance.10,12 Obesity is a major determinant of serum C-reactive protein (CRP) concentrations.13 Studies have also demonstrated that CRP is a major player in the atherosclerotic process at all stages.14-16
Although childhood obesity is found to be associated with increased cardiovascular risk, little is known about the children who are at risk for overweight. The aim of this study was to evaluate inflammation and endothelial dysfunction and its association with insulin resistance in children who were at risk for overweight.
SUBJECTS AND METHODS
Subjects
The study group included 21 children at risk for overweight, defined as a BMI between the 85th and 94th percentile for age and sex according to BMI reference curves for Turkish children.5 The control group included 20 children with a BMI value between the 25th and 74th percentile according to BMI reference curves for Turkish children. The age of the studied subjects ranged from 6 to 17 years. The exclusion criteria were presence of symptoms associated with or detection of infection during basic physical examination, diabetes, familial hyperlipidemia, hypertension, chronic disease and smoking. None of the children had a positive family history for cardiovascular diseases. Color-doppler echocardiography (General Electric, Vivid-3) evaluation was performed in all children with a 3S probe. Children with evidence of structural or functional cardiovascular abnormalities were excluded. The study plan was approved by the local ethics committee and informed consent was obtained from parents.
Methods
Anthropometric parameters including height, weight and waist circumference were evaluated under fasting conditions with the subjects in light clothing and barefoot. These measurements were performed on the same day with brachial artery ultrasonography and echocardiography. Height was measured to the nearest centimeter using a rigid stadiometer. Weight was measured to the nearest 0.1 kg utilizing a calibrated balance scale. BMI was calculated as weight in kilograms divided by the height in meters squared. Waist Circumference (WC) was measured with a steel measuring tape at the highest point of the iliac crest to the nearest 0.1 cm at minimal respiration that corresponded to the end of normal expiration.
Systolic and diastolic blood pressures were measured using a mercury sphygmomanometer after the subject had been seated for 30 min. The average of two measurements taken on the right arm was recorded.
FMD was performed according to the protocol described by Zhu et al.17 In brief, FMD was assessed utilizing a high-resolution ultrasound (Siemens, Sonoline G50) with a probe of 10 mHz. FMD assays were performed by the same expert radiologist. The children were put to rest in a quiet room for at least 15 minutes prior to evaluation of FMD. FMD value was expressed as the percentage change in the brachial artery diameter from baseline to the condition of hyperemia that was achieved after the release of a suprasystolic occlusion. Suprasystolic occlusion was performed 2 cm above the antecubital fossa of the left upper arm. The brachial artery diameter measurements were taken twice from the anterior to the posterior wall of the lumen, such that the first measurement was performed during diastole at baseline and the latter being performed 60 seconds after the release of a 50–mmHg suprasystolic blood pressure cuff occlusion that lasted for 5 minutes.
Blood samples were obtained after an overnight fasting. The blood sample was obtained between 8:00-9:00 via the cannulated antecubital vein. Serum and platelet-poor plasma were obtained by centrifugation at 2000 g at a temperature of 4 °C for 15 minutes. The samples were subsequently stored at -80 °C until assayed.
The levels of serum total cholesterol, HDL cholesterol, triglyceride, uric acid and fasting blood glucose were measured by a colorimetric method using Integra 800 automatic immunoanalyzer (Roche Diagnostic Systems, Mannheim, Germany). Fibrinogen analysis was performed according to the Clauss method.18 The intra-assay and inter-assay variation for the fibrinogen assay were 2.7% and 5.1%, respectively. Low density lipoprotein (LDL) was calculated according to Friedewald’s formula. Fasting insulin levels were determined by a chemiluminescent method (Roche Diagnostics, Mannheim, Germany) utilizing an automatic immunoanalyzer. Serum CRP levels were measured via immunometric assay by Immulite 2000 using high sensitivity CRP kits (Diagnostic Products Corporation, Los Angeles, US). The cut-off value for hsCRP was assigned as 0.10 mg/l. The maximum intra-assay and inter-assay coefficients of variation were 4% and 8.7%, respectively. The homeostasis model assessment of insulin resistance (HOMA-IR) was calculated as fasting serum insulin (μU/ml) x fasting plasma glucose (mmol/l)/22.5 and was used as an index of insulin resistance. In addition, the insulin sensitivity for each subject was calculated with the Quantitative insulin sensitivity check index (QUICKI) formula as 1/ [log (insulin [mU/l]) + log (glucose [mg/dl])].
Statistical analysis
Sample size determination used a significance level of 0.05 for a two-tailed test with 80% power based on previous data regarding obese children. The sample size was calculated using Power and Precision software (Biostat, US). Variable distributions were assessed by the Kolmogorov-Smirnov normality test. According to the variable distribution, the Student t-test or Mann Whitney U test was used for comparison of groups. Categorical variables were compared by using the chi-square test. Correlation analyses were performed using Spearman’s or Pearson’s coefficients according to distribution of the variable. Linear regression analysis was employed to assess correlations between studied parameters. Statistical significance level was set at 0.05.
RESULTS
Median ages for the study group and the healthy controls were 10.5 and 10 years, respectively. Age and sex distribution did not differ in the two groups (Table 1, p >0.05). Significantly higher values of weight, BMI and waist circumference were noted in the study group compared to controls. Children at risk for overweight had higher birth weight (p <0.05). Systolic and diastolic blood pressures were comparable in the two groups. The children in the study group had slightly elevated levels of total cholesterol, triglyceride and LDL cholesterol, and decreased levels of HDL cholesterol compared to controls. However, the differences in these parameters did not reach statistical significance except for the difference in HDL-C which was suggestive. Significantly higher levels of fasting insulin were observed in the study group compared to controls, while fasting glucose values were comparable. HOMA-IR index was significantly higher in the children who were at risk for overweight. They also had a lower QUICKI score; however, the difference between groups was not statistically significant. Serum uric acid and plasma fibrinogen levels did not differ significantly between groups, while serum CRP levels were significantly higher in children at risk for overweight. The children who were at risk for overweight had a lower FMD value compared to children with normal BMI percentiles; however, this difference did not reach statistical significance (Table 1 ).
Four children had reached puberty in each group. However, the differences observed in our study were statistically significant even if the data were adjusted for puberty. Nevertheless, there was a positive correlation between HOMA-IR and age (Figure 1).
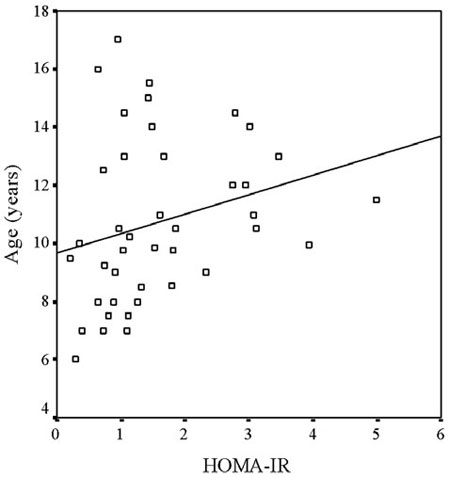
Figure 1. Positive correlation between HOMA-IR and age (r=0.373, p= 0.016).
HOMA-IR index was positively correlated with age, weight, BMI and waist circumference (Table 2 ). Waist circumference was a significant predictor of HOMA-IR index even after adjustment for age and BMI (Table 3 ). Correlation analysis did not reveal any statistically significant relationships between serum CRP levels and other variables (Table 2) .
DISCUSSION
The children at risk for overweight had higher levels of serum CRP and higher values of insulin resistance indices. Although these children had a decreased percentage of FMD and more atherogenic lipid profiles, differences did not reach statistical significance. Waist circumference was the main predictor of insulin resistance in these children.
Obesity is a well known major factor in the development of insulin resistance. Obesity, especially abdominal obesity, has a negative impact on insulin sensitivity.19 The Framingham study20 has clearly shown that increasing weight is associated with an increased incidence of cardiovascular events in adults. Insulin resistance is considered to be a strong predictor of cardiovascular disease even in the absence of glucose intolerance.21 Elevated plasma insulin concentrations after an oral glucose tolerance test have been found to be an independent predictor of coronary artery disease in the Paris Prospective Study.22 Insulin resistance is associated with the development of risk factors for atherosclerosis including an atherogenic lipid profile and endothelial dysfunction.2 Sinaiko et al8 found that insulin resistance at age 13 years predicts systolic blood pressure and triglyceride levels at age 19 years. The association between obesity and insulin resistance is not only related to age and sex specific BMI percentiles but may also be related to fat distribution. Central obesity, which can be assessed by waist circumference measurement, has been found to be associated with insulin resistance more frequently than peripheral body fat distribution.2,21
Elevated concentration of CRP is an independent risk factor for cardiovascular disease.16 CRP levels are increased in childhood obesity.23 Data from the Third National Health and Nutrition Examination Survey (NHANES-III) have demonstrated that the CRP levels are elevated in children of the higher percentiles of BMI.24 The Cardiovascular Risk in Young Finns Study25 has shown that the direct correlation between hs-CRP and carotid intima-media thickness is driven by the effects of adiposity. A relationship between obesity and inflammation possibly explains the high levels of CRP in obesity.13 Despite adequate data from studies in childhood obesity, our findings of higher CRP levels and impaired insulin sensitivity in children who are at risk for overweight are novel. The Expert committee has recommended that prolonged weight stabilization is an appropriate goal for children over 7 years if their BMI is between the 85th and 94th percentiles and if they have no secondary complications of obesity.1 However, the data of our study suggest that being at risk for overweight per se may be associated with some alterations in inflammation and insulin resistance which can lead to high risk for cardiovascular disorders.
We must note that our work has some limitations. 1) The study sample size is small for the investigation of a relationship between variables, thus the lack of statistical significance in terms of FMD values between groups may be due to inadequate sample size. 2) We evaluated insulin resistance by calculating HOMA-IR from fasting serum insulin and plasma glucose values, whereas the gold standard for investigating and quantifying insulin resistance is the hyperinsulinemic euglycemic clamp.26 Despite these limitations we were able to demonstrate a significant difference in insulin resistance between the groups. However, the HOMA-IR values calculated in children at risk for overweight in the present study were under the cut-off levels, which indicate insulin resistance in obese children.27 3) Finally, our study is of a cross-sectional design. A prospective follow-up study may provide more reliable data.
In conclusion, we found that there are some alterations in insulin resistance and inflammation in those children who are at risk for overweight. It can thus be assumed that children who are at risk for overweight may also be at risk for atherosclerosis as much as obese children. We suggest that, as for the obese children, a relatively aggressive treatment strategy should also be adopted for those children who are at risk for overweight, aiming at obesity and atherosclerosis prevention.
ACKNOWLEDGEMENTS
The authors thank Dr. Ruveyda Bundak for providing BMI charts of Turkish children.
REFERENCES:
1. Barlow SE, Dietz WH, 1998 Obesity evaluation and treatment: Expert Committee recommendations. The Maternal and Child Health Bureau, Health Resources and Services Administration and the Department of Health and Human Services. Pediatrics 102: E29.
2. Weiss R, Dziura J, Burgert TS, et al, 2004 Obesity and the metabolic syndrome in children and adolescents. N Engl J Med 350: 2362-2374.
3. U.S. Preventive Services Task Force, 2006 Screening and interventions for overweight in children and adolescents: recommendation statement. Am Fam Physician 73: 115-119.
4. Ogden CL, 2004 Defining overweight in children using growth charts. Md Med 5: 19-21.
5. Bundak R, Furman A, Gunoz H, et al, 2006 Body mass index references for Turkish children. Acta Paediatr 95: 194-198.
6. Ells LJ, Campbell K, Lidstone J, et al, 2005 Prevention of childhood obesity. Best Pract Res Clin Endocrinol Metab 19: 441-454.
7. Smoak CG, Burke GL, Webber LS, et al, 1987 Relation of obesity to clustering of cardiovascular disease risk factors in children and young adults. The Bogalusa Heart Study. Am J Epidemiol 125: 364-372.
8. Sinaiko AR, Steinberger J, Moran A, et al, 2006 Influence of insulin resistance and body mass index at age 13 on systolic blood pressure, triglycerides, and high-density lipoprotein cholesterol at age 19. Hypertension 48: 730-736.
9. Sinaiko AR, Steinberger J, Moran A, et al, 2005 Relation of body mass index and insulin resistance to cardiovascular risk factors, inflammatory factors, and oxidative stress during adolescence. Circulation 111: 1985-1991.
10. Meyer AA, Kundt G, Steiner M, Schuff-Werner P, Kienast W, 2006 Impaired flow-mediated vasodilation, carotid artery intima-media thickening, and elevated endothelial plasma markers in obese children: the impact of cardiovascular risk factors. Pediatrics 117: 1560-1567.
11. Ross R, 1986 The pathogenesis of atherosclerosis–an update. N Engl J Med 314: 488-500.
12. Garanty-Bogacka B, Syrenicz M, Syrenicz A, Gebala A, Walczak M, 2005 Relation of acute-phase reaction and endothelial activation to insulin resistance and adiposity in obese children and adolescents. Neuro Endocrinol Lett 26: 473-479.
13. Park HS, Park JY, Yu R, 2005 Relationship of obesity and visceral adiposity with serum concentrations of CRP, TNF-alpha and IL-6. Diabetes Res Clin Pract 69: 29-35.
14. Ridker PM, 2001 High-sensitivity C-reactive protein: potential adjunct for global risk assessment in the primary prevention of cardiovascular disease. Circulation 103: 1813-1818.
15. Rutter MK, Meigs JB, Sullivan LM, D’Agostino RB Sr, Wilson PW, 2004 C-reactive protein, the metabolic syndrome, and prediction of cardiovascular events in the Framingham Offspring Study. Circulation 110: 380-385.
16. Koenig W, Sund M, Frohlich M, et al, 1999 C-Reactive protein, a sensitive marker of inflammation, predicts future risk of coronary heart disease in initially healthy middle-aged men: results from the MONICA (Monitoring Trends and Determinants in Cardiovascular Disease) Augsburg Cohort Study, 1984 to 1992. Circulation 99: 237-242.
17. Zhu W, Huang X, He J, Li M, Neubauer H, 2005 Arterial intima-media thickening and endothelial dysfunction in obese Chinese children. Eur J Pediatr 164: 337-344.
18. Clauss A, 1957 [Rapid physiological coagulation method in determination of fibrinogen]. Acta Haematol 17: 237-246.
19. Weiss R, Caprio S, 2005 The metabolic consequences of childhood obesity. Best Pract Res Clin Endocrinol Metab 19: 405-419.
20. Hubert HB, Feinleib M, McNamara PM, Castelli WP, 1983 Obesity as an independent risk factor for cardiovascular disease: a 26-year follow-up of participants in the Framingham Heart Study. Circulation 67: 968-977.
21. Chew GT, Gan SK, Watts GF, 2006 Revisiting the metabolic syndrome. Med J Aust 185: 445-449.
22. Fontbonne AM, Eschwege EM, 1991 Insulin and cardiovascular disease. Paris Prospective Study. Diabetes Care 14: 461-469.
23. Cook DG, Mendall MA, Whincup PH, et al, 2000 C-reactive protein concentration in children: relationship to adiposity and other cardiovascular risk factors. Atherosclerosis 149: 139-150.
24. Ford ES, Galuska DA, Gillespie C, et al, 2001 C-reactive protein and body mass index in children: findings from the Third National Health and Nutrition Examination Survey, 1988-1994. J Pediatr 138: 486-492.
25. Kivimaki M, Lawlor DA, Juonala M, et al, 2005 Lifecourse socioeconomic position, C-reactive protein, and carotid intima-media thickness in young adults: the cardiovascular risk in Young Finns Study. Arterioscler Thromb Vasc Biol 25: 2197-2202.
26. Radikova Z, 2003 Assessment of insulin sensitivity/resistance in epidemiological studies. Endocr Regul 37: 189-194.
27. Keskin M, Kurtoglu S, Kendirci M, Atabek ME, Yazici C, 2005 Homeostasis model assessment is more reliable than the fasting glucose/insulin ratio and quantitative insulin sensitivity check index for assessing insulin resistance among obese children and adolescents. Pediatrics 115: e500-503.
Address for correspondence:
Baris Akinci, Division of Endocrinology of Metabolism, Department of Internal Medicine,
University of Dokuz Eylul, Inciralti, 35340
Izmir, Turkey, Tel.: +90-232-4123744, Fax: +90-232-2792267, e-mail: baris.akinci@deu.edu.tr
Received 12-07-07, Revised 10-10-07, Accepted 20-12-07