Abstract
OBJECTIVE: Leptin is primarily produced in adipose tissue and appears to play a modulatory role between metabolism and immunity. Given that obesity, a state of chronic inflammation, is an established risk factor for Renal Cell Carcinoma (RCC), we investigated the association between plasma leptin levels and RCC risk. DESIGN: This case-control study included 70 patients with newly diagnosed, histologically confirmed RCC and 280 age-, gender- and district of residence-matched controls. Anthropometric data, socio-demographic variables, medical history, lifestyle habits and dietary data were derived from a personal interview. Serum leptin and adiponectin levels were determined using standard commercial kits. Adjusted odds ratios for RCC risk were derived through multiple logistic regression analyses. RESULTS: Leptin levels were inversely associated with RCC risk (OR: 0.53, CI: 0.28- 0.99, p = 0.05), even after controlling for potential confounding factors, such as Body Mass Index (BMI), recent weight change, history of diabetes mellitus and other obesity related hormones, notably adiponectin. CONCLUSIONS: The precise mechanism linking obesity with RCC remains unclear; however, the inverse association of leptin with RCC might be attributed, at least in part, to hormonal cross-talk with complex neuron-endocrine and immune circuits. These findings, if confirmed in prospective and interventional studies, might further elucidate the underlying mechanisms.
Obesity, a state of chronic, low-grade systemic inflammation, is an established risk factor for Renal Cell Carcinoma (RCC), a rather immunogenic tumor.1 Furthermore, cross-talk between lymphocytes and adipocytes may contribute to immune regulation. Indeed, adipose tissue produces a variety of proinflammatory and anti-inflammatory factors, including leptin, adiponectin, as well as cytokines, such as Tumor Necrosis Factor-α (TNF-α) and Interleukin-6 (IL-6).2,3
Apart from leptin’s impact on energy homeostasis, important functions for the regulation of immunocompetence have also been unraveled. A role of leptin in immune modulation is further strengthened by the hormone’s structural similarities to cytokines and the high homology of Ob-Rb to members of the class I cytokine receptor family.4,5
Previous studies have shown that increased leptin levels and over-expression of leptin receptors were associated with RCC invasion.6-8 Given the immunogenic character of RCC and the evident role of leptin in the modulation of the immune system, we hypothesized that leptin may be implicated in the development of this tumor.
SUBJECTS AND METHODS
Subjects
From October 2002 to May 2005, 70 patients with newly diagnosed, histologically confirmed RCC were recruited from four collaborating hospitals in the Athens metropolitan area. None of the patients had been previously diagnosed with any other malignancy or chronic disease. For each patient, four controls matched for gender, age (±5 years) and district of residence in the Athens metropolitan area, were consecutively enrolled in the investigation. Exclusion control criteria comprised self-reported medical history of cancer, hepatic disease, major hormonal or hematological disorders, asthma, autoimmune disease, HIV infection, advanced heart failure, chronic kidney failure, recent myocardial infarction, stroke, acute pancreatitis or bone fracture. Five controls refused to be recruited; on the other hand, all patients agreed to participate, while 10 patients with other than RCC histology were excluded. The study protocol was approved by the University of Athens Medical School Ethics Committee and written informed consent was obtained from the subjects prior to study enrolment.
Methods
Trained health professionals interviewed the participants on the basis on a pre-coded questionnaire including socio-demographic, anthropometric, lifestyle and medical history variables. Anthropometric variables (height, weight, waist and hip circumference) were measured with standard techniques.9,10 In order to collect information on dietary intake and to assess the average frequency of the consumption of indicated portion sizes of different food or beverage items, including coffee and alcohol, we used a validated, previously described, food frequency questionnaire.11-13 For the purpose of the study we created two food type groups: the vegetarian diet category consisting of cereals and starchy roots, sugars and syrups, pulses, nuts and seeds, vegetables and fruits, and the protein diet category comprising meat and meat products, fish and seafood, milk and dairy products. In order to assess the degree of exercise among study subjects, the frequency and duration of different categories of physical activities during leisure time was also recorded (in minutes/day).
Fasting morning blood samples were obtained and properly stored for hormonal and glucose measurements. Determinations were performed blindly as to case-control status in the Beth Israel Deaconess Medical Center, in Boston, USA. Leptin, a stable analyte, was assayed by RIA (Lincoln Research, Inc., St Charles, MO, USA; sensitivity 0.5 ng/ml; intra-assay CV 3.4–8.3%).14 Adiponectin levels were measured by immunoassay; sensitivity 2 ng/ml; intra-assay CV <10%, as previously described.9
Statistical analysis
For the statistical analyses, representative values of the anthropometric variables, leptin/adiponectin levels and dietary data were calculated among cases and controls and the t-test was used to assess the direction and significance of the difference in the numeric studied variables between RCC patients and controls. Differences in the distribution of categorical variables between cases and controls were tested using Pearson’s Chi-square or Fisher’s exact test. The Pearson’s correlation coefficient of leptin with several parameters was assessed to identify possible predictors of hormones levels among controls. To study the association of leptin with RCC, we modelled the data through univariate and multivariate conditional logistic regression models. We used case-control as the outcome variable and leptin, as well as a series of possible confounders, as predictor variables, namely Body Mass Index (BMI), weight loss two months prior to diagnosis, Waist to Hip Ratio (WHR), education, physical exercise, smoking habit, coffee consumption, alcohol consumption, self-reported history of diabetes mellitus (DM) or fasting glucose level higher than 125 mg/dl, intakes of protein and vegetarian diet groups and adiponectin. Data were analysed using the SAS.15
RESULTS
The study included patients aged 22-83 years (mean value = 62, SD = 13.6) and controls 23-87 years (mean value = 61, SD = 14.1), 60% of whom were males. Leptin levels by tumor characteristics are presented in Table 1 . Stage IV RCC patients had significantly lower leptin levels compared with stage I patients. The risk for stage I vs. stage IV RCC, also controlling for age, gender, BMI and WHR, was over twofold higher for an increment of 1 SD of leptin levels (OR = 2.66, CI: 1.11- 6.39, p = 0.03).
Tables 2a and 2b show anthropometric, demographic, lifestyle, hormonal and medical history variables by case-control status. Leptin and adiponectin levels were lower among RCC cases compared to controls (p = 0.04 and 0.06, respectively). Mean values of BMI were not significantly different between cases and controls (p = 0.69); however, mean values of WHR and weight change were significantly higher among cases (p < 0.001 and 0.02, respectively). RCC patients consumed fewer vegetarian products when compared with controls (p <0.001), whereas no significant difference was observed concerning protein products. RCC patients, when compared with controls, were of lower educational level, had lower physical activity patterns (p = 0.02 and 0.001, respectively) and had more frequently a history of DM (p = 0.01). Alcohol consumption seemed to exert a bimodal pattern with RCC, with moderate drinkers over-represented among controls and those who either abstain or consume more than one drink per day (p = 0.001).
To examine the associations of leptin with age and individual anthropometric variables, the Pearson correlation coefficients among healthy controls were calculated (Table 3 ). Leptin was positively and statistically significantly correlated with age, BMI and weight change. Lastly, a non-significant association with WHR, adiponectin, protein and vegetarian diet was also noted. These results may not be directly interpretable because of the possibility of mutual confounding.
Subsequently, crude and adjusted odds ratios for RCC were calculated for each increment of leptin, corresponding to one standard deviation among controls (Table 4 ). The unadjusted odds ratio for leptin was 0.65 (95% CI = 0.42- 0.99, p = 0.04) and remained statistically significant after controlling for BMI, recent weight change, WHR, education level, physical activity, smoking, coffee and alcohol consumption, protein and vegetarian diet, DM and adiponectin.
DISCUSSION
An excess RCC risk was observed among patients with low circulating levels of leptin, after adjusting for potential confounding factors, such as central obesity, DM and adiponectin. Increased leptin levels have been associated with carcinogenesis in several organs, however, the mechanisms by which obesity promotes cancer development remain unknown.10,16-19
In our study, leptin levels were inversely associated with RCC risk and this association could be attributed in part to the weight loss due to disease; however, the dataset comprised newly diagnosed cases of RCC and the inverse association of leptin with RCC remained stable, even after controlling for confounding factors, including weight change. Therefore, we considered this association as primary. Given the immunogenic nature of RCC and the evident role of leptin in the regulation of immunocompetence, we opted to propose a theoretical pathogenetic mechanism that may link obesity, a state of chronic inflammation, with the immune system through leptin’s inter-talk with complex neuro-endocrine and other neural and immune circuits (Figure 1).
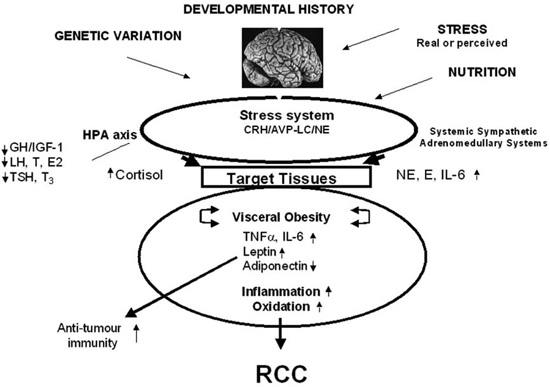
Figure 1. Theoretical model of the pathogenetic pathways linking Leptin with RCC. Obesity is associated with high TNF-α, high IL-6 and high leptin levels derived from fat. All three factors are proinflammatory and hence increase inflammation and oxidation. Oxidation is pro-tumor while leptin potentially has increased anti-tumor immunity effect. Obesity is also associated with low adiponectin, which has anti-tumour and anti-inflammatory properties, thus facilitating tumor growth and increased systemic inflammation. The protective effect of leptin on RCC is suggested by our findings.
CRH: corticotropin- releasing hormone, AVP: arginine vasopressin, LC: locus coeruleus, NE: norepinephrine, HPA: hypothalamicpituary-adrenal, GH: growth hormone, IGF-1: insulin- like growth factor-1, LH: luteinizing hormone, T: testosterone, E2: estradiol, RCC: Renal Cell Carcinoma, TSH: thyroid stimulating hormone, T3: triiodothyronine, E: epinephrine, IL-6: interleukin-6, TNF-α: tumor necrosis factor-α.
Leptin influences both innate and adaptive immunity.2,4,5 In obesity, monocytes/macrophages infiltrate adipose tissue and secrete proinflammatory cytokines, such as TNF-α and IL-6, which in turn stimulate adipocytes to further secrete proinflammatory and anti-inflammatory adipo-cytokines, such as leptin and adiponectin.2,5 Leptin and the hypothalamic-pituitary-adrenal axis have reciprocal effects on inflammation.20 Catecholamines also exhibit a stimulatory effect on IL-6 and suppress leptin secretion.21 Alterations in the energy metabolism, as well as of the immune system, as expressed by excessive production of proinflammatory cytokines, might lead to oxidation and thus to carcinogenesis.5,22
RCC is an immunogenic tumor, as indicated by the results of non-specific immunotherapy based on Interferon-alpha (IFN-α) and Interleukin-2 (IL-2).23 Down-regulation or loss of HLA molecules has been documented among RCC patients, providing evidence of a strategy that these tumors may use in order to evade T-cell mediated immunosurveillance. In addition, a tumor-specific up-regulation of Human Leukocyte Antigen-G (HLA-G), leading to an impaired immune response, has recently been described in RCC. HLA-G expression in RCC cells in vivo as well in vitro can possibly lead to impaired immune recognition by cytotoxic T lymphocytes, natural killer and lymphokine activated killer cells, and may play a role in their escape from immunosurveillance mechanisms.24
Experimental studies did not document leptin-induced growth in RCC lines, whereas other studies have shown that increased leptin levels and over-expression of leptin receptors were associated with RCC invasion.6-8 Moreover, leptin exerts an anti-cancer effect by induction of NK cells proliferation and activation.25-27 It has also been reported that the proinflammatory state of obesity may induce an attenuated response of immune competent cells to an acute endogenous or exogenous leptin challenge and inhibit the promigratory and activating effects of a leptin challenge on NK cells.28 These reports along with the results of the present study support the hypothesis that obesity may lead to impaired immune functions and that low leptin levels among RCC patients suggest reduction or loss of leptin’s anti-tumour effect (Figure 1).
This study has several strengths including the exclusion of renal cancer cases with different underlying pathophysiology and the blinded evaluation in one batch of the serum analytes. Selection bias cannot be excluded as in any case-control study; however, the educational level of the control group was similar to that of the study area population. Among the inherent limitations of the study design is the inability to measure pre-diagnosis levels of leptin or other cytokines/hormones mentioned in the theoretical model as well as the lack of the time sequence criterion for causality. These findings may stimulate further large prospective trials also aiming at exploring the underlying mechanisms of RCC.
ACKNOWLEDGMENTS
We thank T Kakkavas, K Livadas, S Papadoukakis, A Zarogiannos, I Liakatas, G Papadopoulos, A Paschalis, M Angelopoulos, S Gialamas, T Katsifotis and A Pagonis for their valuable contribution. The project has been Supported in part by the University of Athens Medical School.
REFERENCES
1. Lipworth L, Tarone RE, McLaughlin JK, 2006 The epidemiology of renal cell carcinoma. J Urol 176: 2353-2358.
2. Matarese G, Moschos S, Mantzoros CS, 2005 Leptin in Immunology. J Immunol 173: 3137-3142.
3. Shamsuzzaman AS, Winnicki M, Wolk R, et al, 2004 Independent association between plasma leptin and C-reactive protein in healthy humans. Circulation 109: 2181-2185.
4. De Rosa V, Procaccini C, Gaetano C, et al, 2007 A key role of leptin in the control of regulatory T cell proliferation. Immunity 26: 241-255.
5. La Cava A, Alviggi C, Matarese G, 2004 Unraveling the multiple roles of leptin in inflammation and autoimmunity. J Mol Med 82: 4-11.
6. Horiguchi A, Sumitomo M, Asakuma J, et al, 2006 Increased serum levels and over expression of leptin receptors are associated with the invasion and progression of renal cell carcinoma. J Urol 176: 1631-1635.
7. Horiguchi A, Sumitomo M, Asakuma J, et al, 2006 Leptin promotes invasiveness of murine renal cancer cells via extracellular signal-regulated kinases and rho dependent pathway. J Urol 176: 1636-1641.
8. Attoub S, Noe V, Pirola L, et al, 2000 Leptin promotes invasiveness of kidney and colonic epithelial cells via phosphoinositide 3-kinase-, rho-, and rac-dependent signaling pathways. Faseb J 14: 2329-2338.
9. Spyridopoulos TN, Petridou E.Th, Skalkidou A, et al, 2007 Low adiponectin levels are associated with renal carcinoma: A case-control study. Int J Cancer 120: 1573-1578.
10. Gogas H, Trakatelli M, Dessypris N, et al, 2008 Melanoma risk in association with serum leptin levels and lifestyle parameters: a case-control study. Ann Oncol 19: 384-389.
11. Gnardellis C, Trichopoulou A, Katsouyanni K, Polychronopoulos E, Rimm EB, Trichopoulos D, 1995 Reproducibility and validity of an extensive semiquantitative food frequency questionnaire among Greek school teachers. Epidemiology 6: 74–77.
12. Petridou E, Kedikoglou S, Koukoulomatis P, et al, 2002 Diet in relation to endometrial cancer risk: a case-control study in Greece. Nutr Cancer 44: 16-22.
13. Petridou E, Ntouvelis E, Dessypris N, Terzidis A, Trichopoulos A, the Childhood Hematology-Oncology Group, 2005 Maternal diet and acute lymphoblastic leukemia in young children. Cancer Epidemiol Biomarkers Prev 14: 1935-1939.
14. Gavrila A, Chan JL, Yiannakouris N, et al, 2003 Serum adiponectin levels are inversely associated with overall and central fat distribution but are not directly regulated by acute fasting of leptin administration in humans: cross-sectional and interventional studies. J Clin Endocrinol Metab 88: 4823-4831.
15. SAS Institute Inc. 1989 SAS/ STAT User’s Guide, Version 6, 4th Ed. Cary NC.
16. Petridou E, Papadiamantis Y, Markopoulos C, et al, 2000 Leptin and insulin growth factor I in relation to breast cancer (Greece). Cancer Causes Control 11: 383-388.
17. Petridou E, Belechri M, Dessypris N, et al, 2002 Leptin and body mass index in relation to endometrial cancer risk. Ann Nutr Metab 46: 147-151.
18. Stattin P, Lukanova A, Biessy C, et al, 2004 Obesity and colon cancer: does leptin provide a link? Int J Cancer 109: 149-152.
19. Stattin P, Soderberg S, Hallmans G, et al, 2001 Leptin is associated with increased prostate risk: a nested case-referent study. J Clin Endocrinol Metab 86: 1341-1345.
20. Steiner AA, Romanovsky AA, 2007 Leptin: At the crossroads of energy balance and systemic inflammation. Prog Lipid Res 46: 89-107.
21. Pinkney JH, Coppack SW, Mohamed-Ali V, 1998 Effect of isoprenaline on plasma leptin and lipolysis in humans. Clin Endocrinol 48: 407-411.
22. Federico A, Morgillo F, Tuccillo C, et al, 2007 Chronic inflammation and oxidative stress in human carcinogenesis. Int J Cancer 121: 2381-2386.
23. Parker A, Cerhan JR, Lynch CF, et al, 2004 History of Urinary Tract Infection and Risk of Renal Cell Carcinoma. Am J Epidemiol 159: 42-48.
24. Bukur J, Malenica B, Huber C, Seliger B, 2003 Altered expression of nonclassical HLA class 1B antigens in human renal cell carcinoma and its association with impaired immune response. Human Immunology 64: 1081-1092.
25. Hu X, Juneja SC, Maihle NJ, et al, 2002 Leptin: a growth factor in normal and malignant breast cells and for normal mammary gland development. J Natl Cancer Inst 94: 1704-1711.
26. Oelmann E, Haghgu S, Kulimova E, et al, 2003 Re: Leptin: a growth factor in normal and malignant breast cells and for normal mammary gland development. J Natl Cancer Inst 95: 1171-1173.
27. Elinav E, Abd-Elnabi A, Pappo O, et al, 2006 Suppression of hepatocellular carcinoma growth in mice via leptin, is associated with inhibition of tumor cell growth and natural killer cell activation. J Hepatol 44: 529-536.
28. Nave H, Mueller G, Siegmund B, et al, 2008 Resistance of JAK-2 dependent leptin signaling in NK cells – a novel mechanism of NK cell dysfunction in diet-induced obesity. Endocrinology doi:10.1210/en.2007-1516.
Address for correspondence:
Eleni Th. Petridou, Professor of Preventive Medicine and Epidemiology, Department of Hygiene,
Epidemiology and Medical Statistics, Athens University Medical School, 75 Mikras Asias Str,
Goudi, Athens 11527, Greece, Tel.: +30 210 7462187, Fax: +30 210 7462105, e-mail: epetrid@med.uoa.gr
Received 05-06-08, Revised 10-09-08, Accepted 30-10-08