Abstract
OBJECTIVE: The aim of the study was to describe the clinical, biochemical, and genetic features of a sample of Mediterranean patients with RTH (resistance to thyroid hormone) due to mutations in TRβ (thyroid hormone receptor beta) referred to our institution during the last 15 years. DESIGN: 166 blood samples were received for RTH genetic testing between January 1997 and December 2011. Genetic testing was performed by PCR amplification followed by sequencing of exons 7, 8, 9, and 10. Clinical and biochemical features were obtained from available information sent by referring hospitals. RESULTS: Mutations were identified in 50 patients (29 probands and 21 relatives). 64% were women, and mean±stdev age at diagnosis among probands was 33.2±20.5 years. The following clinical features were recorded: goiter in 50%, hyperkinetic behavior in 32%, and tachycardia in 29%. Up to 19% of the probands had undergone some type of thyroidal ablative therapy before diagnosis. As for biochemical features, mean±stdev TSH was 10.2±21.4 mUI/L, and mean±stdev fT4 was 35.5±10.8 pmol/L. We found four new mutations: p.Phe451Leu, p.Pro452Arg, p.Glu457Gly, and p.Phe459Leu. CONCLUSIONS: The clinical and biochemical characteristics of our samples of Mediterranean populations with RTH were similar to those described in the published literature. Interestingly, in our populations we have identified four novel mutations in the TRβ gene.
INTRODUCTION
Resistance to thyroid hormones (RTH) is a genetic disorder, first described by S. Refetoff in 1967,1 characterized by high-serum free T4 concentration and non-suppressed TSH.2-5 The prevalence of this disease is about 1:40000 births,6 and it is caused in 85% of cases by heterozygous mutations in the thyroid hormone receptor beta (TRβ) gene,2,3 although there are a few cases due to homozygous TRβ mutations.7-9 Recently, the firsts patients with mutation in thyroid hormone receptor-α (TRα) have been described, with clinical features similar to those of congenital hypothyroidism and displaying a different biochemical pattern, characterized by near-normal thyroid hormone levels but a subnormal ratio of thyroxine to triiodothyronine and low reverse triiodothyronine levels.10,11
There are nearly 400 families worldwide diagnosed with RTH presenting more than 130 different mutations2 (Online Mendelian Inheritance in Man (OMIM) and HGMD® databases). The medical literature includes some series of RTH patients,12-14 but most data come from North-American studies.2 The scarce information about a Mediterranean population is comprised in a paper published by Beck-Peccoz which refers to Italy.3 To date, the Spanish population is scarcely mentioned in the medical literature, with only case reports15 or small series of patients.16
Against this background, the aim of our study was to describe the clinical, biochemical, and genetic features of samples of Mediterranean populations with especial emphasis on the Spanish population with RTH by mutations in the TRβ gene referred to our institution for genetic testing during the last 15 years.
SUBJECTS AND METHODS
We reviewed all the samples sent to our Institution (one of the referral centers in Spain) for genetic testing of mutations in TRβ from January 1997 to December 2011. The decision to perform the genetic study was made by physicians of the referring hospital. We excluded the samples of patients from non-Mediterranean countries. Even though it is generally accepted that 15% of RTH patients have no mutations in the TRβ gene, (2, 3, 16) only those patients with confirmed mutation were included in the analysis to avoid diagnostic errors.
Clinical and biochemical features were obtained from available information sent by referring hospitals. We recorded the existence of goiter, hyperkinetic behavior, and tachycardia, as well as the previous use of anti-thyroidal drugs, beta-blockers, L-T4, and any type of thyroidal ablation (radioiodine or thyroidectomy). The biochemical features analyzed were: TSH, free thyroxine, and thyroidal autoimmunity (anti-thyroperoxidase and anti-thyroglobulin antibodies).
Informed consent was obtained to perform genetic testing. Genomic DNA from the patients was isolated from peripheral blood using a commercial kit (QIAamp DNA Mini Kit, Qiagen, Hilden, Germany). Exons 7, 8, 9, and 10 and their flanking intronic regions were amplified by PCR using specific primers. The resulting PCR products were visualized on a 2% agarose gel prior to direct sequencing using the Big-Dye terminator cycle sequencing reaction kit (Applied BioSystems, Foster City, CA). All the mutations obtained were compared with those previously described in MEDLINE (OVID) and HGMD® databases.
RESULTS
We received 170 samples for genetic testing of mutations in TRβ; of these, four were excluded from this analysis because they belonged to non-Mediterranean individuals. Among the remaining 166 samples (164 Spanish and 2 Greek patients), mutations were identified in 50 patients (29 probands and 21 relatives), representing 30.1% of the total. 64% of patients with mutation in TRβ were women, and mean±stdev age at diagnosis among probands was 33.2±20.5 years (range: 1.5-82 years), with 31% of patients being aged ≤20 years at the time of diagnosis. The rest of the baseline characteristics are shown in Table 1.
The following clinical features were recorded among patients with TRβ mutation: goiter in 50%, hyperkinetic behavior in 32%, and tachycardia in 29% of patients. Anti-thyroidal drugs were used in 19%, beta-blockers in 9.5%, and L-T4 in 9.5% of the patients. Up to 19% of the probands had undergone some type of thyroidal ablative therapy (radioiodine or thyroidectomy) before diagnosis.
Regarding the biochemical features of the individuals with mutation, the mean±stdev TSH was 10.2±21.4 mUI/L (NV 0.4-4 mUI/L), with 33.3% of our patients having TSH above the upper normal limit. Regarding the fT4, the mean±stdev was 35.5±10.8 pmol/L (or 2.75±0.84 ng/dL) (NV 10.3-25.8 pmol/L), with 88.8% of our patients having fT4 above the upper normal limit. We had information of anti-thyroidal autoimmunity in only 12 of 50 patients, 16.7% of whom were positive.
Genetic testing yielded 25 different heterozygote mutations in TRβ. All of them except one (p.Arg383Cys) were in the three hot regions of the TRβ gene previously described by S. Refetoff.2 The most common mutation in these samples was that of p.Arg243Gln, harbored by three unrelated families. Interestingly, regarding the mutation p.Arg338Trp, which is the most common in the published series, only one of our patients presented it. Furthermore, we have identified four new mutations (16% of all the mutations), all of them single nucleotide substitutions. The four new mutations were located in exon 10 (p.Phe451Leu, p.Pro452Arg, p.Glu457Gly and p.Phe459Leu) (Figure 1).
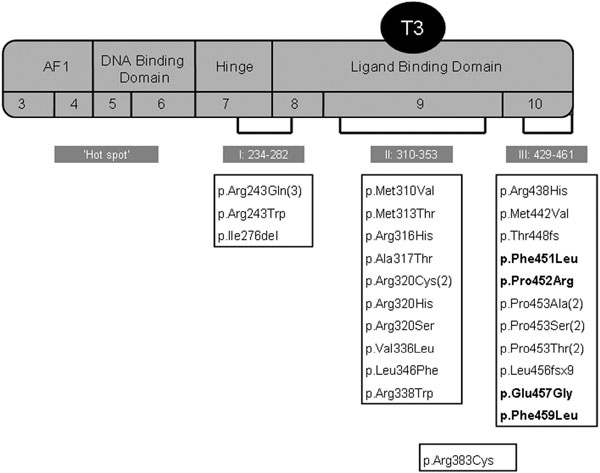
Figure 1. Mutations of TRβ gene in our series. The number of different families sharing the same mutation are shown in brackets. New mutations are shown in bold. AF1, ligand-independent activation function.
DISCUSSION
This study shows that clinical and biochemical features of our samples of Mediterranean populations with RTH by mutations in the TRβ gene are similar to those previously described in other series, while genetic features differ remarkably, with our identification of four new mutations in TRβ.
RTH is a disease mainly caused by mutations in the TRβ gene,2-5 although in recent years mutations in TRα have been associated with a different phenotype.10,11 In about 15% of patients with a confirmed clinical and biochemical pattern of RTH, no mutations of the TRβ gene have been identified;2,3,17 involved mechanisms might be mutations in co-activator or co-repressor proteins18 or mosaicism.19 Nevertheless, our rate of positive genetic testing is only 30.1% of all samples, and 21.3% among probands. Most likely this discrepancy is due to an inadequate selection of cases in which other possible causes of a biochemical pattern suggesting RHT should be ruled out.
Regarding clinical features, our findings in confirmed RTH are similar to those observed in previous series,2,13 goiter being the most common clinical trait. Age at diagnosis is another remarkable feature, about one third being identified among pediatric patients. By contrast, one unusual case of our series was diagnosed at 82 years; this delay may be attributed to the indolent nature of this condition, which leads to the development of mild symptoms in most patients.
In general, treatment is not warranted in RHT unless signs and symptoms of hypo- or hyperthyroidism develop.20 The first situation requires LT4 replacement therapy, while treatment of the second condition is more controversial, with good results recently reported via administration of 3,5,3’-triiodothyroacetic acid.21 On the other hand, misdiagnosis of RTH is quite common, leading to unnecessary treatments such as thyroidectomy or radioiodine, followed thereafter by lifelong replacement therapy.22 In this connection, special mention must be made of the high proportion of our patients who had undergone thyroidal ablative treatments prior to diagnosis (19%), a figure that has not improved since previous series published 15-20 years earlier.13
The association between RTH and autoimmune thyroid disease is well documented.23 Gavin et al24 suggested that chronic TSH stimulation in RTH activates intra-thyroidal lymphocytes to produce the pro-inflammatory cytokine TNF-alpha, leading to thyroid cell destruction by binding to its receptors on thyrocytes, or indirectly by potentiating antibody formation or cytotoxic T lymphocyte production. This hypothesis, however, has recently been rejected,23 and the link between RTH and thyroid autoimmunity has yet to be elucidated. In our study, the prevalence of anti-thyroidal autoimmunity was 16.7%, lower than that reported by Barkoff et al,23 which was about 22%. On the other hand, autoimmunity in our series may be underestimated, as autoantibodies were reported in just 25% of all cases.
The genetic features of our sample of Mediterranean populations with RTH differ notably from other Mediterranean and non-Mediterranean series.2,3,12,13 Our most common mutation was p.Arg243Gln (first described by Yagi H et al25), harbored by three unrelated families, located in exon 7 and corresponding to the hinge domain of TRβ. The most frequent mutation in the other series, p.Arg338Trp, located in exon 9 and corresponding to the T3-binding domain was present in only one patient. It should be underlined that almost 10% of our mutations are deletions or insertions, double the 5% reported in the literature. In addition, we identified four new mutations in exon 10, all of them in the hot regions of the molecule and located in the T3-binding domain (p.Phe451Leu, p.Pro452Arg, p.Glu457Gly and p.Phe459Leu).
Our study has several limitations. As clinical features were obtained from the information sent by referring institutions, we could not describe them thoroughly and analysis is therefore limited to the most frequently reported items, such as goiter, hyperkinetic behavior, and tachycardia. Moreover, we could not estimate the prevalence of RTH without mutation in the TRβ gene because we could not rule out misdiagnosis, as relevant information from most of these patients was lacking.
In conclusion, we report the clinical, biochemical, and genetic features of our samples of Mediterranean populations, with particular focus on Spanish patients, and describe four novel mutations in the TRβ as a cause of RTH.
DISCLOSURE
The authors have no conflict of interest to disclose.
REFERENCES
1. Refetoff S, DeWind LT, DeGroot LJ, 1967 Familial syndrome combining deaf-mutism, stuppled epiphyses, goiter and abnormally high PBI: possible target organ refractoriness to thyroid hormone. J Clin Endocrinol Metab 27: 279-294.
2. Refetoff S, Dumitrescu AM, 2007 Syndromes of reduced sensitivity to thyroid hormone: genetic defects in hormone receptors, cell transporters and deiodination. Best Pract Res Clin Endocrinol Metab 21: 277-305.
3. Beck-Peccoz P, Persani L, Calebiro D, Bonomi M, Mannavola D, Campi I, 2006 Syndromes of hormone resistance in the hypothalamic-pituitary-thyroid axis. Best Pract Res Clin Endocrinol Metab 20: 529-546.
4. Refetoff S, Weiss RE, Usala SJ, 1993 The syndromes of resistance to thyroid hormone. Endocr Rev 14: 348-399.
5. Beck-Peccoz P, Mannavola D, Persani L, 2005 Syndromes of thyroid hormone resistance. Ann Endocrinol (Paris) 66: 264-269.
6. Lafranchi SH, Snyder DB, Sesser DE, et al, 2003 Follow-up of newborns with elevated screening T4 concentrations. J Pediatr 143: 296-301.
7. Usala SJ, Menke JB, Watson TL, et al, 1991 A homozygous deletion in the c-erbA beta thyroid hormone receptor gene in a patient with generalized thyroid hormone resistance: isolation and characterization of the mutant receptor. Mol Endocrinol 5: 327-335.
8. Takeda K, Sakurai A, DeGroot LJ, Refetoff S, 1992 Recessive inheritance of thyroid hormone resistance caused by complete deletion of the protein-coding region of the thyroid hormone receptor-beta gene. J Clin Endocrinol Metab 74: 49-55.
9. Ferrara AM, Onigata K, Ercan O, Woodhead H, Weiss RE, Refetoff S, 2012 Homozygous thyroid hormone receptor β-gene mutations in resistance to thyroid hormone: three new cases and review of the literature. J Clin Endocrinol Metab 97: 1328-1336.
10. Bochukova E, Schoenmakers N, Agostini M, et al, 2012 A mutation in the thyroid hormone receptor alpha gene. N Engl J Med 366: 243-249.
11. Van Mullem A, van Heerebeek R, Chrysis D, et al, 2012 Clinical Phenotype Associated with Mutation of Thyroid Hormone Receptor-α1 (TRα1). Endocr Rev 2: 33(03_MeetingAbstracts): OR26-1.
12. Adams M, Matthews C, Collingwood TN, Tone Y, Beck-Peccoz P, Chatterjee KK, 1994 Genetic analysis of 29 kindreds with generalized and pituitary resistance to thyroid hormone. Identification of thirteen novel mutations in the thyroid hormone receptor beta gene. J Clin Invest 94: 506-515.
13. Brucker-Davis F, Skarulis MC, Grace MB, et al, 1995 Genetic and clinical features of 42 kindreds with resistance to thyroid hormone. The National Institutes of Health Prospective Study. Ann Intern Med 123: 572-583.
14. Rivolta CM, Olcese MC, Belforte FS, et al, 2009 Genotyping of resistance to thyroid hormone in South American population. Identification of seven novel missense mutations in the human thyroid hormone receptor beta gene. Mol Cel Probes 23: 148-153.
15. Gómez JJL, Pomar MDB, Casariego AV, Rodríguez IC, 2009 Selective pituitary resistance to thyroid hormone in a patient treated with amiodarone. Endocrinol Nutr 56: 418-421.
16. Lado Abeal J, Albero Gamboa R, Araujo Vilar D, et al, 2011 Clinical and molecular study of five families with resistance to thyroid hormones. Med Clin (Barc) 137: 551-554.
17. Vlaeminck-Guillem V, Margotat A, Torresani J, D’herbomez M, Decoulx M, Wémeau JL, 2000 Resistance to thyroid hormone in a family with no TRbeta gene anomaly: pathogenic hypotheses. Ann Endocrinol (Paris) 61: 194-199.
18. Reutrakul S, Sadow PM, Pannain S, et al, 2000 Search for abnormalities of nuclear corepressors, coactivators, and a coregulator in families with resistance to thyroid hormone without mutations in thyroid hormone receptor beta or alpha genes. J Clin Endocrinol Metab 85: 3609-3617.
19. Mamanasiri S, Yesil S, Dumitrescu AM, et al, 2006 Mosaicism of a thyroid hormone receptor-beta gene mutation in resistance to thyroid hormone. J Clin Endocrinol Metab 91: 3471-3477.
20. Weiss RE, Refetoff S, 1999 Treatment of Resistance to Thyroid Hormone–Primum Non Nocere. J Clin Endocrinol Metab 84: 401-404.
21. Anzai R, Adachi M, Sho N, Muroya K, Asakura Y, Onigata K, 2012 Long-term 3,5,3’-triiodothyroacetic acid therapy in a child with hyperthyroidism caused by thyroid hormone resistance: pharmacological study and therapeutic recommendations. Thyroid 22: 1069-1075.
22. Mohammed IA, Aldasouqi S, Schnute R, Refetoff S, Weiss RE, Iqbal N, 1998 The syndrome of resistance to thyroid hormone, misdiagnosed and treated as thyrotoxicosis. Endocr Pract 4: 391-395.
23. Barkoff MS, Kocherginsky M, Anselmo J, Weiss RE, Refetoff S, 2010 Autoimmunity in patients with resistance to thyroid hormone. J Clin Endocrinol Metab 95: 3189-3193.
24. Gavin C, Meggison H, Ooi TC, 2008 Proposing a causal link between thyroid hormone resistance and primary autoimmune hypothyroidism. Med Hypotheses 70: 1024-1028.
25. Yagi H, Pohlenz J, Hayashi Y, Sakurai A, Refetoff S, 1997 Resistance to thyroid hormone caused by two mutant thyroid hormone receptors beta, R243Q and R243W, with marked impairment of function that cannot be explained by altered in vitro 3,5,3’-triiodothyroinine binding affinity. J Clin Endocrinol Metab 82: 1608-1014.
Address for correspondence:
Antonio J. Amor, Endocrinology and Nutrition Department, Hospital Clinic i Universitari, Villarroel 170, 08036 Barcelona, Spain, Tel.: 34 932279846, Fax: 34 934516638, e-mail: ajamor@clinic.ub.es
Received 12-10-2012, Accepted 03-04-2013