HORMONES 2005, 4(4):213-220
DOI: 10.14310/horm.2002.——
Address correspondence and requests for reprints to:
Kalliopi Pazaitou-Panayiotou, 2 Al. Simeonidis Str., 54007 Thessaloniki, Greece
Received 30-07-05, Revised 20-09-05, Accepted 10-10-05
Abstract
OBJECTIVE: To define clinical presentation, surgical complications, follow-up characteristics, and survival of 23 children and adolescents with thyroid carcinoma. DESIGN: Retrospective analysis of data of 23 children and adolescents with thyroid carcinoma cared for in the Theagenion Cancer Hospital, Thessaloniki. RESULTS: At the time of diagnosis cervical lymph node metastases were present in 18 (78.2%), mediastinal in 2 (8.69%), and pulmonary in 3 patients (13%). Total thyroidectomy was performed in 21 patients, with lymph node dissection in 18 and subtotal thyroidectomy in 2. No significant post-operative complications were observed. Histological examination revealed differentiated thyroid carcinoma (DTC). Tumor was multifocal in 11 (47.8%) and bilateral in 7 subjects (63.6%). Thyroid capsule invasion, vascular invasion, soft tissue involvement, and parathyroid gland invasion was observed in 12 out of 23 patients (52.1%). All patients received thyroxine suppressive therapy and 21 of them additional therapy with radioactive iodine (131I). During follow-up (5.5 years), 6 out of the 23 patients presented new metastases in the cervical and mediastinal lymph nodes, lungs, and bones. At last follow-up, 11 patients (47.8%) had residual disease but all were alive. CONCLUSIONS: Thyroid carcinoma in children and adolescents can be quite aggressive. When a young patient presents thyroid nodule or multinodular goiter or palpable lymph nodes, the existence of thyroid carcinoma must be seriously considered.
Key words: Thyroid carcinoma, Adolescents, Children, Lung metastases
INTRODUCTION
Thyroid carcinoma is a rare disease in the first two decades of life. It is estimated that 10% of the total cases of thyroid carcinoma occur within this age range.1 It is very rare before the age of 10, its incidence increasing with age.2 Childhood thyroid carcinoma has a female predominance, with a female to male ratio of 2.5-6 to 1.0.3 Several studies have shown that thyroid carcinoma in pediatric patients differs from that in adults with respect to its presentation and outcome. Although pediatric patients with thyroid carcinoma tend to present with disease at a more advanced stage than adults, namely a higher incidence of lymph nodes and pulmonary metastases, the prognosis is better for them.4,5 Guidelines with regards to optimal management of DTC in children and adolescents are based primarily on the experience of a few specialists of tertiary care academic Institutions.6 Hence the description of additional cohorts of pediatric DTC patients is of intrinsic value. In this communication, we present our data on 23 children and adolescents with thyroid carcinoma. The study is retrospective and includes mode of presentation, clinical course, and long-term outcome of therapy. It is important to underline that this study refers to a genetically relatively homogeneous population. All patients were born in Northern Greece and the exposure of the presented cases to environmental iodine loads was most probably similar. Data were analyzed in an anonymized fashion. No medullary thyroid carcinoma cases are included in this study.
SUBJECTS AND METHODS
Twenty-three children and adolescents (15 females and 8 males) aged 8 to 20 (mean 15.9±3.3) years were treated for differentiated thyroid carcinoma (DTC) in the Theagenion Cancer Hospital from 1987 to 2004. The main presenting symptoms were a solitary thyroid nodule in 12 and multinodular goiter in 7. Palpable cervical lymph nodes were present in 14 of them, and a palpable lateral cervical mass with normal thyroid in 4 patients. No patient had received head or neck external radiation therapy. One patient had a family history of papillary thyroid carcinoma. Fine needle aspiration bi
opsy (FNAB) was performed in 4 patients and led to the diagnosis of thyroid carcinoma. In 2 patients the diagnosis was established after biopsy of an enlarged lymph node, and in 17 the diagnosis was established by histology after thyroidectomy.
Total thyroidectomy was performed in 21, with unilateral cervical lymph node dissection in 18 patients, and lymph node dissection of the upper mediastinum in 2 of them. Subtotal thyroidectomy was performed in 2 patients carrying a small cold node (0.5 and 0.9cm in diameter, respectively). After surgery one patient presented transient hypoparathyroidism, but no patient presented recurrent laryngeal nerve damage. Postoperatively, ablation therapy with 80-100 mCi of radioactive 131I was given in 21/23 patients in order to eradicate any remaining normal or malignant thyroid tissue. Ablation therapy was not given in the 2 patients with subtotal thyroidectomy. Thyroid hormone therapy was applied in all patients.
A whole body scan (WBS) was performed 4-7 days after ablation therapy. TSH and thyroglobulin (Tg) measurement in the hypothyroid condition was carried out in all patients by IRMA methods (Brahms and Schering, respectively).
RESULTS
Histology revealed papillary thyroid carcinoma (PTC) in 21/23 patients (91.3%), with pure papillary type in 13 (61.9%) and papillary TC-follicular variant in 8 (38.1%). In the remaining 2 patients follicular carcinoma and insular carcinoma, respectively were detected (Table 1 ). Tumor size ranged from 0.23 to 5 cm (maximum diameter); 9 children had tumors measuring <1.5 cm. Multiple tumor foci of the papillary type were detected in 11 patients47.8%), with bilateral location in 7 of them (63.6%). Thyroid capsule invasion, vascular invasion, soft tissue involvement, and parathyroid gland invasion were observed in 12/23 (52.1%). Multiple cervical lymph node metastases were observed in 18 patients (78.2%), with unilateral involvement in 12 (66.6%) and bilateral in 6 patients (33.3%). Moreover, mediastinal lymph node metastases were present in 2 patients (8.69%) (Table 2).
Postoperatively, on discontinuing L-thyroxine for ablation therapy with radioactive iodine, serum Tg levels ranged from 0.1 to 4237 ng/ml, and TSH from 52.8 to140 µU/ml (normal range 0.3-4 ìU/ml). At the time of diagnosis of thyroid cancer, pulmonary metastases were present in 3 patients, diagnosed by the WBS, carried out 4-7 days after ablation therapy. One of them had mediastinal metastasis as well (Table 2). Tg levels of these patients are presented in Figure 1. None of the patients received either external beam radiotherapy or chemotherapy for disease control.
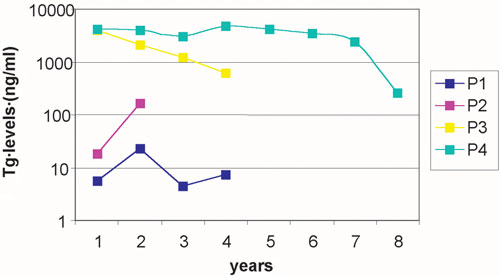
Figure 1. Tg levels (ng/ml) during follow-up in four patients (P1, P2, P3, P4) who had distant metastases at the time of diagnosis of the thyroid carcinoma. P1 had mediastinal metastasis, P2 had simultaneously lung and mediastinal metastases, P3 and P4 had lung metastasis. The square symbols indicate time of 131I administration during follow-up.
In 2 patients, subtotal thyroidectomy was performed because of a small cold nodule. Pathology revealed a papillary microcarcinoma 0.5 and 0.9 cm in diameter, respectively with no signs of infiltration or extension beyond the nodule capsule. High resolution ultrasonography of the remaining thyroid lobe showed a normal thyroid with no nodular disease. No further surgery was recommended.7 In these 2 patients no ablation therapy was given. Tg on thyroxine in these two patients was undetectable, and in hypothyroid condition was 5ng/ml and remained stable during the follow-up period of 10 yrs and 17 yrs, respectively.
Classification of the disease in all patients according to the TNM system8 is shown in Table 3 .
FOLLOW-UP DATA
The mean duration of follow-up was 5.5 years (range 1.3 to 17 years). The patients were followed by clinical examination, thyroid and neck ultrasonography, TSH, FT4, and serum Tg levels every 6 months in order to detect recurrence or progression of the disease. WBS with radioactive 131I or computed tomography (CT) were performed when necessary.
During the follow-up, between 12 and 72 months (mean 37.33 months) after the ablation therapy, 6 of the 23 patients (26%) presented with local recurrences or new metastases (Table 4 ). Two of them presented cervical lymph node recurrences, two mediastinal lymph node metastases, one lung and cervical node metastases, and one patient skull metastasis, mediastinal lymph node metastases, and lung metastases (Table 4 ). Even patients with tumor size £1.5cm eventually presented with distant metastases (Figure 2). Two of the above-mentioned patients, who presented cervical node recurrences, were re-operated on. All patients who had residual disease after the ablation therapy or presented new metastases received additional doses of radioactive iodine therapy. Thus, 7 patients received 100-150 mCi of radioactive 131I as an additional dose because of residual local disease or mediastinal lymph node metastases, 4 received 200-350 mCi in 2 additional doses due to lung metastases, and one (female) received 1150 mCi in 7 additional doses due to persistent lung metastases. No severe complications (such as second malignancy, pulmonary fibrosis or decreased fertility in male patients) were observed as a result of high cumulative doses of radioactive 131I therapy. All residual diseases or metastases were either histologically proven or had positive WBS and elevated Tg (>5 ng/ml).
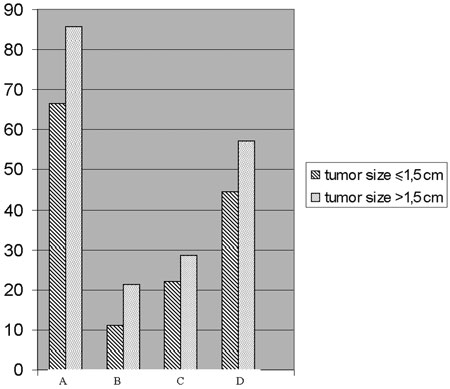
Figure 2. Patients (%) with metastases according to tumor size. A: Cervical lymph node metastases at diagnosis. B: Distant metastases at diagnosis. C: Newly developed distant metastases during the follow-up. D: Free of disease at last follow-up.
At last follow-up, 12 patients (52.2%) were in complete remission (Table 6 ). Ten of them, those with total thyroidectomy, had undetectable Tg levels under thyroxine therapy and Tg<1 ng/ml under hypothyroid condition, negative WBS, and normal cervical ultrasonography. Two patients with subtotal thyroidectomy had normal thyroid and cervical ultrasonography, undetectable Tg under thyroxine therapy, or Tg<5 ng/ml in hypothyroid condition. Eleven patients (47.8%) had residual disease (Table 5 ), but all were alive and asymptomatic.
DISCUSSION
Although most cases of thyroid carcinoma (TC) occur in adults, TC may occur in children and adolescents, and it is generally agreed that its occurrence and clinical course are different from those of the adult. Children present larger tumors and a greater incidence of lymph node metastases9 at presentation but the prognosis is much better.9,10 Nevertheless, thyroid carcinoma can on rare occasions be a lethal neoplasm.9,11 Genetic factors, complex immune patterns of antitumor or peritumoral fibrosis, variable angiogenic responses, sensitivity to ambient levels of ionizing radiation between children and adults, late diagnosis, and other unknown factors, are probably responsible for the generally encountered greater extend of the disease at presentation in children. Patients who present lymph nodes and lung metastases usually require higher doses of radioactive 131I.
The female to male ratio in our patients was 2.12 to 1. When the analysis was limited to prepubertal patients, the gender ratio was close to unity, but when older adolescents are included in pediatric series, as in our study, a greater prevalence of females to males is observed.3,12 The disease is presented as solitary thyroid nodule or multinodular goiter with cervical lymph nodes involvement in the majority of patients. The reported malignancy in cases of solid, cold thyroid nodule ranges from 17 to 36% in young people.13-15 In 4 of our patients a palpable lateral cervical mass was observed which proved to be metastasis of papillary thyroid carcinoma, while the thyroid gland appeared clinically normal. In these patients total thyroidectomy was performed and revealed a 0.6-1 cm papillary thyroid carcinoma.
Histology revealed papillary carcinoma in 91.3% of our patients, follicular in 4.34%, and insular in 4.34%. Similar distributions have been reported by other authors.16 Although papillary carcinoma is rare under the age of 10, two of our patients aged 8 and 9 years had papillary thyroid carcinoma. One of them presented metastases in lung and skull one year after the diagnosis of the disease and was treated with additional doses of 131I. 47.8% of our patients had multifocal disease and in 63.6% of them involvement of both lobes was observed. Similar results were reported by Segal et al.17 Cervical lymph nodes metastases were present in 18/23 (78.2%) of our patients at the time of diagnosis. This rate is higher than that reported by Mc Henry et al.12 Lung metastases in different reports is variable, ranging from 6 to 25%.12,18,19 Three out of the 23 patients (13%) had pulmonary metastases at the time of diagnosis, and 2 presented pulmonary metastasis during the follow-up. Even small tumors (<1.5 cm) generated local or distant metastases. None of our patients had bone metastasis at diagnosis, but our youngest patient (8 years old) with papillary carcinoma developed cranial bone metastasis one year after the diagnosis of thyroid carcinoma.
Capsular invasion, soft tissue invasion, and positive margins, were observed at diagnosis in the majority of our patients who later presented with recurrent or metastatic disease, and these characteristics must be considered significant prognostic factors of recurrences or metastases in patients with thyroid carcinoma.20 However, it must be stressed that one patient with papillary thyroid carcinoma developed lymph node metastasis in the mediastinum 5 years after the diagnosis of the disease, despite the fact that its initial lesion was not infiltrative.
The optimal management of thyroid carcinoma in children and adolescents has not as yet been defined. Most cases can be cured by a combination therapy which include surgery and radioactive iodine.21 Surgery is the initial treatment for all cases. Some authors suggest that subtotal thyroidectomy and thyroid hormone suppressive therapy are effective in controlling disease restricted to one lobe. The majority of the authors, however, recommend total or near-total thyroidectomy,22 selective lymph node dissection when neck metastases are present, ablation therapy with radioactive 131I, and thyroid hormone suppressive therapy23,24 In view of the fact that DTC are often bilateral and multifocal in origin,4,17 we apply in our center total thyroidectomy as the treatment of choice. The reported high rate of lesions to the laryngeal nerve and postoperative hypoparathyroidism4 were infrequent complications in our series and must be so in general if patients are referred to specialized surgeons. Total thyroidectomy was performed in 21/23 patients with cervical lymph node dissection in 18 of them. Only one of our patients presented transient hypoparathyroidism. The extent of cervical lymph node dissection is an important issue. All clinically involved lymph nodes are dissected. But local recurrences or metastases are a common problem in young patients with DTC. Therefore, complementary surgery may be necessary to eradicate recurrences or metastases. Two of our patients who presented cervical lymph node metastases (18 and 60 months after ablation therapy) were re-operated.
Twenty-one of our 23 patients (91.3%) have received additional therapy with radioactive 131I. Larger doses were necessary to treat lymph nodes and lung metastases. One patient received 1230 mCi for persistent metastatic lung disease. We administered fixed-therapy doses of 131I to our patients. Whether one should adjust these doses for body surface or body weight in children, assuming an average body surface of 1.72 m2 and body weight of 70 kg for adults, remains controversial. Hung and Sarlis6 propose that if fixed doses of 131I are to be used in pediatric patients, these should be derived by adjusting the corresponding 131I activities given for therapy in adults, taking into account the body surface and total body weight of the younger patients as proposed by Reynolds.25 Radioactive iodine treatment has been found to be safe and effective in the management of metastases.26 High doses of radioactive iodine, frequently used in patients with lung metastases, may increase the risk of pulmonary fibrosis,27 but this can probably be avoided when there are intervals between therapies. The risk of induction of a secondary solid tumor after iodine therapy in later life though small does exist. Vassilopoulou-Sellin et al11 have found a 7% incidence of radioiodine_related secondary malignancies over the following decades. Large doses of 131 I may cause acute myeloid leukemia and bladder cancer. Decreased fertility has been reported in male patients after high cumulative doses of radioactive iodine.28,29 The two patients with papillary carcinoma who underwent subtotal thyroidectomy have not received ablation therapy. They had small size TC, no infiltrative disease, and good differentiation. No recurrence or metastases have been observed during the follow-up (120 and 204 months, respectively). All patients received suppressive doses of L-thyroxine, and were monitored by serum thyroglobulin levels, WBS, and ultrasonography.
Tg in the hypothyroid condition has been established as a sensitive tumor marker,30,31 especially when measured by the most up-to-date assays. Detectable or elevated levels of thyroglobulin indicate persistent, recurrent or metastatic disease. Elevated serum Tg levels were observed in 5 of our 6 patients with DTC, who presented new metastasis. Pediatric patients generally tolerate poorly thyroid hormone withdrawal and induced hypothyroidism. Recombinant human TSH (rhTSH), an exogenous source of human TSH, has been introduced in clinical practice as an effective alternative to thyroid hormone withdrawal for the follow-up of DTC patients.32 rhTSH is effective in promoting Tg release in thyroid cancer cells, without inducing hypothyroidism. The use of rhTSH has not been approved for diagnostic purposes in pediatric patients, although it is safe and yields the same results in children and adolescents as in adult patients. The optimal dose of rhTSH has not yet been defined, but seems to be similar to that used in adults.33 If rhTSH is to be administered, patients receive one injection of rhTSH (0.9 mg im, Thyrogen) for 2 consecutive days. Serum Tg is measured before and after rhTSH stimulation (days 4 and 5). Even minor increases from undetectable baseline serum Tg may be associated with recurrent or metastatic disease.34
Survival rates of 86-100% are reported in young patients with thyroid carcinomas.8,9,19 At last follow-up, all patients were alive but 11 still had residual disease (Table 5). Considering the indolent course of DTC, this is a relatively short time of median follow-up (5.5 years). Local or distant metastases can occur and must be recognized and treated promptly. When children present a cold nodule or multinodular goiter, or a palpable cervical mass, pediatricians must be alerted to the possible existence of thyroid carcinoma.
The follow-up time must be extended to a life-long period so that more reliable conclusions can be drawn. Although pediatric survival rates are long-term, DTC in children and adolescents should be considered as a potentially lethal disease. Moreover, the risk of induction of a secondary solid tumor after iodine therapy in later life though small nevertheless exists.
In summary, children and adolescents who are presented with advanced thyroid carcinoma have overall a good prognosis. Total thyroidectomy and lymph nodes dissection is the treatment of choice, along with therapy with radioactive 131I. Tg in the lympothyroid state is a sensitive tumor marker.
REFERENCES
1. Millman B, Pelliteri PK, 1995 Thyroid Carcinoma in Children and Adolescents. Arch Otoraryngol Head Neck Surg 121: 1261-1264.
2. Wiersinga WM, 2001 Thyroid Cancer in Children and Adolescents _ Consequences in later life. J Pediatr Endocrinol Metab 14: Suppl 5: 1289-1298.
3. Schlumberger M, Pacini F, 2003 Childhood and pregnancy. In: Schlumberger M, Pacini F (eds) Thyroid tumor, Nucleon, Paris; pp, 219-225.
4. Massimino M, Gasparini M, Ballerini E, Del Bo R, 1995 Primary thyroid carcinoma in children: a retrospective study of 20 patients. Med Pediatr Oncol 24: 13-17.
5. Gorlin JB, Sallen SE, 1990 Thyroid cancer in childhood. Endocrinol Metab Clin North Am 19: 649-662.
6. Hung W, Sarlis N, 2002 Current controversies in the management of pediatric patients with well-differentiated nonmedullary thyroid cancer: a review. Thyroid 12: 683-702.
7. Hay ID, Grant CS, Van Heerden JA, Goellner JR, Ebersold JR, Bergstralh EJ, 1992 Papillary thyroid microcarcinoma. a study of 535 cases observed in a 50-year period. Surgery 112: 1139-1147.
8. AJCC, 2002 Thyroid. In: AJCC (ed) Cancer Staging handbook, Springer-Verlog, New York; pp, 89-98.
9. Zimmerman D, Hay ID, Gough IR, et al, 1988 Papillary thyroid carcinoma in children and adults: long-term follow-up of 1039 patients conservatively treated at one institution during three decades. Surgery 104: 1157-1166.
10. Goepfert H, Dichtel WJ, Samaan NA, 1984 Thyroid cancer in children and teenagers. Arch Otolaryngol 110: 72-75.
11. Vassilopoulou-Sellin R, Goepfert U, Raney B, Schultz PN, 1998 Differentiated thyroid cancer in children and adolescents: clinical outcome and mortality after long-term follow-up. Head Neck 20: 549-555.
12. Lamberg BA, Karkinen-Jaaskelainen M, Franssila KO, 1989 Differentiated follicle-derived thyroid carcinoma in children. Acta Paediatr Scand 78: 419-425.
13. Flannery TK, Kirkland JL, Copeland KC, Bertuch AA, Karaviti LP, Brandt ML, 1996 Papillary Thyroid Cancer: a Pediatric Perspective. Pediatrics 98: 464-466
14. McHenry C, Smith M, Lawrence AM, Jarosz H, Paloyan E, 1988 Nodular thyroid disease in children and adolescents: a high incidence of carcinoma. Am Surg 54: 444-447.
15. Halac I, Zimmerman D, 2005 Thyroid nodules and cancers in children. Endocrinol Metab Clin North Am 34: 725-744.
16. Kumar A, Bal CS, 2003 Differentiated thyroid cancer. Indian J Pediatr 70: 707-713.
17. Segal K, Hadar T, Lubin E, Abraham A, Levy R, 1992 Thyroid carcinoma in children and adolescents. Harefuah 122: 83-86.
18. Ceccarelli C, Pacini F, Lippi F, et al, 1988 Thyroid cancer in children and adolescents. Surgery 104: 1143-1148.
19. Giuffrida D, Scollo C, Pellegriti G, et al, 2002 Differentiated thyroid cancer in children and adolescents. J Endocrinol Invest 25: 18-24.
20. Grigsby P, Gal-or A, Michalski J, Doherty G, 2002 Childhood and adolescent thyroid carcinoma. Cancer 95: 724-729.
21. Leboulleux S, Baudin E, Hartl DW, Travagli JP, Schlumberger M, 2005 Follicular cell-derived thyroid cancer in children. Horm Res 63: 145-151.
22. Thompson GB, Hay ID, 2004 Current strategies for surgical management and adjuvant treatment of childhood papillary thyroid carcinoma. World J Surg 28: 1187-1198.
23. Jocham A, Joppich I, Hecker W, Knorr D, Schwarz HP, 1994 Thyroid carcinoma in childhood: management and follow-up of 11 cases. Eur J Pediatr 153: 17-22.
24. Feinmesser R, Lubin E, Segal K, Noyek A, 1997 Carcinoma of the thyroid in children_a review. J Pediatr Endocrinol Metab 10: 561-568.
25. Reynolds JC, 1993 Comparison of I-131 absorbed radiation doses in children and adults: a tool for estimating therapeutic I-131 doses in children. In: Robbins J (ed) Treatment of Thyroid Cancer in Childhood, DOE Publication, Washington, DC; pp, 127-135.
26. Samuel AM, Sharma SM, 1991 Differentiated Thyroid Carcinomas in Children and Adolescents. Cancer 8: 2186-2190.
27. Van Nostrand D, Neutze J, Atkins F, 1986 Side effects of “rational dose” iodine-131 therapy for metastatic well differentiated thyroid carcinoma. J Nucl Med 27: 1519-1527.
28. Pacini F, Gasperi M, Fugazzola L, et al, 1994 Testicular function in patients with differentiated thyroid carcinoma treated with radioiodine. J Nucl Med 35: 1418-1422.
29. Mazzaferri EL, Klools RT, 2001 Current approaches to primary therapy for papillary and follicular thyroid cancer. J Clin Endocrinol Metab 86: 1447-1463.
30. Damiani D, Dichtchekenian V, Setian N, et al, 2001 Thyroid carcinoma in children and adolescents _ review of six cases. J Pediatr 77: 45-48.
31. Shah DH, Dandekar SR, Jeevanram RK, Kumar A, Sharma SM, Ganatra RD, 1981 Serum thyroglobylin in differentiated thyroid carcinoma: Histological and metastatic classification. Acta Endocrinol 98: 222-226.
32. Iorcansky S, Herzovich V, Qualey RR, Tuttle RM, 2005 Serum TSH levels following recombinant human TSH injections in children and teenagers with papillary thyroid cancer. J Clin Endocrinol Metab (Epub ahead of print).
33. Duntas LH, Tsakalakos N, Grab-Duntas B, Kalarritou M, Papadodima E, 2003 The use of recombinant human thyrotropin (Thyrogen). Hormones 2: 169-174.
34. Pacini F, Molinaro E, Lippi F, et al, 2001 Prediction of disease status by recombinant human TSH-stimulated serum Tg in the postsurgical follow-up of differentiated thyroid carcinoma. J Clin Endocrinol Metab 86: 5686-5690.