HORMONES 2007, 6(3):227-232
DOI: 10.14310/horm.2002.——
Address for correspondence:
George Kontogeorgos M.D., Ph.D., Department of Pathology (Anatomic Pathology), General Hospital of Athens, KOFKA Building, 1st Floor, 154 Messogion Avenue, 115 27 Athens, Greece, Tel./Fax: +30 210 7784302, e-mail: gkonto@med.uoa.gr
Received 08-12-06, Revised 03-03-07, Accepted 10-04-07
Abstract
OBJECTIVE: Galectin-3 (Gal-3) belongs to the family of carbohydrate-binding proteins with high affinity for galactoside and is involved in many biological processes including cell growth and differentiation, cell adhesion, tumor progression, apoptosis and metastasis. The aim of this study was to disclose differences in the expression of Gal-3 in silent and functioning corticotroph pituitary adenomas. DESIGN: We examined 30 pituitary adenomas (19 functioning corticotroph, 11 silent corticotroph adenomas). Two prolactinomas and 2 functioning somatotroph adenomas served as positive controls. Antigen retrieval was done by three-minute incubation via pressure boiler in citrate buffer solution, pH 6.0. A polymer was used as a secondary link to DAB chromogen. The independent variables t-test was used for comparison of the mean expression of Gal-3 in the two different corticotroph adenoma subgroups. RESULTS: Eighteen of the functioning corticotroph adenomas (94.73%) were positive for Gal-3 with a cytoplasmic and focally membranous distribution; two cases also exhibited nuclear expression, whereas 9 of the silent corticotroph adenomas (81.81%) had zero or <1% expression of Gal-3 (p=0.001). CONCLUSIONS: Gal-3 is highly expressed in functioning corticotroph adenomas of the pituitary gland, while silent adenomas exhibit very focal to null expression of Gal-3. This observation can be used in the pathological diagnosis to separate functioning from silent corticotroph adenomas of the pituitary.
Key words: Corticotroph, Galectin 3, Immunohistochemistry, Pituitary adenoma, Silent adenoma
INTRODUCTION
Galectins are a family of carbohydrate-binding proteins with a high affinity for β-galactoside.1 Gal-3 is one of the most extensively investigated proteins of the 14-member group of galectins involved with β1,3 (4)-galactosylation.2,3 Gal-3 is implicated in cell growth and differentiation, cell adhesion, angiogenesis, tumor progression, apoptosis and metastasis and has been detected in many human tumors and cell lines, including thyroid, colon and breast.4-9 Gal-3 expression was detected by immunohistochemistry and western blot analysis in lactotrophs, corticotrophs and folliculostellate cells of normal human pituitaries; also in corticotroph and lactotroph adenomas and carcinomas.10,11 Recently, a significant difference in Gal-3 expression was found between functioning and silent corticotroph adenomas.11
Nonfunctioning corticotroph adenomas can be diagnosed as silent only when clinical information confirming lack of hypercortisolism is available. Silent corticotroph adenomas are morphologically indistinguishable from ordinary functioning ACTH-producing adenomas by histology, histochemistry and immunohistochemistry. There is, so far, no specific marker to distinguish silent from functioning adenomas.12 Silent subtype 2 corticotroph adenomas can only be differentiated by electron microscopy.13
The aim of this study was to further investigate the role of Gal-3 as an immunohistochemical marker in the differential diagnosis of silent from functioning corticotroph adenomas.
MATERIAL AND METHODS
Thirty pituitary adenomas, 19 functioning corticotroph and 11 silent corticotroph were retrieved from the files of the Pituitary Tumor Reference Center, Department of Pathology, G. Gennimatas Athens General Hospital, Hellas. All patients with functioning corticotroph adenomas were associated with Cushing’s disease and showed elevated serum cortisol levels, whereas those with silent were clinically presented with symptoms related to the tumor mass. The tumors were examined by histology, histochemistry with the periodic acid-Schiff technique, and immunohistochemistry for all adenohypophysial hormones (GH, PRL, ACTH, β-TSH, β-FSH, β-LH α-SU) as described previously.12
Immunohistochemistry for Gal-3 was performed in all corticotroph adenomas, as well as in 2 prolactinomas and 2 functioning somatotroph adenomas; the latter served as positive controls. Sections of 4 to 6 µm thick cut from buffered formalin-fixed, paraffin-embedded tissues were immunostained with Gal-3 monoclonal antibody (Vector Laboratories, Inc., Burlingame CA, dilution 1:500). The one step Envision polymer (Dako A/S, Glostrup, Denmark) was used as a secondary link to DAB chromogen. Before application of the primary antibody, antigen retrieval was carried out by three-minute incubation with a pressure boiler in citrate buffer solution, pH 6.0. Tissue sections from functioning corticotroph adenomas, where citrate buffer substituted the primary antibody, served as negative control. For the independent variables, t-test (SPSS 10) was used for comparing the mean expression of Gal-3 in the two different types of corticotroph adenomas. For further analysis, the non-parametric Mann-Whitney U test was performed.
RESULTS
All 30 tumors were basophilicinroutinestains,PAS positive and typically immunoreactive for ACTH. One functioning adenoma with extensive Crooke’s hyaline deposits in tumor cells was classified as Crooke’s adenoma. Crooke’s hyaline change in corticotroph cells of the adenohypophysial parenchyma fragments included in the specimens were exclusively noted in functioning corticotroph adenomas.
Eighteen functioning corticotroph adenomas (94.73%) expressed Gal-3. The mean percentage of Gal-3 positive adenoma cells was 77% (SD: 31.35%). The distribution of Gal-3 immunoreactivity was diffuse, cytoplasmic and focally membranous (Figure 1a). Negative case control is shown in Figure 1b. Two functioning tumors also exhibited nuclear expression. Marked membranous Gal-3 distribution with nuclear immunostaining was particularly noted in the Crooke’s adenoma (Figure 2). The patient with the Crooke’s adenoma was an 18-yr-old woman, who received external irradiation after surgery and developed panhypopituitarism; her serum cortisol levels dropped to zero. Five years after surgery, the patient is under corticoids replacement therapy with no further complications.
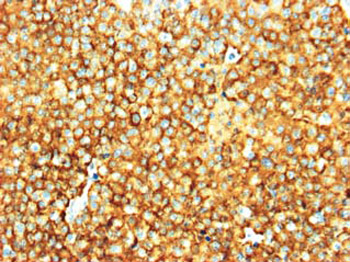
Figure 1a. Strong and diffuse Gal-3 immunoreactivity in a functioning corticotroph adenoma (ABC 20X).
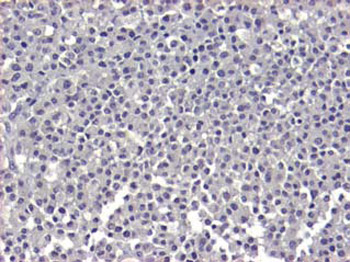
Figure 1b. Negative case control of functioning corticotroph adenoma. The primary antibody was omitted and substituted by buffer solution (ABC 20X).
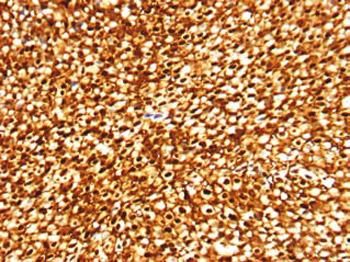
Figure 2. Membranous distribution of Gal-3 with nuclear immunoreactivity in a Crooke’s cell adenoma. The hyaline deposits remain negative (ABC 10X).
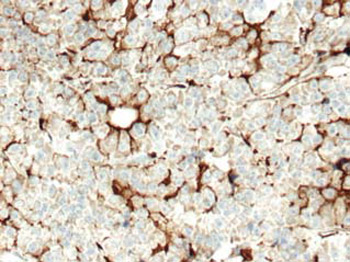
Figure 3. Gal-3 negative silent corticotroph adenoma. Gal-3 reveals and highlights the cytoplasmic processes folliculostellate cells distributed among adenoma cells and focally forming follicles (ABC 20X).
In addition, Gal-3 immunoreactivity highlighted the cytoplasmic processes of scattered folliculostellate cells included in functioning and silent corticotroph adenomas (Figure 3), as well as in the nontumorous adenohypophysial parenchyma. In contrast, among the silent corticotroph adenomas, 9 (81.81%) were completely negative for Gal-3, or were positive in less than 1% of their cell population. The two remaining silent adenomas expressed Gal-3 in 15% and 80% of their tumor cells (overall mean percentage in silent tumors: 8.72%, SD: 24.05%). Our results show statistically significant difference in Gal-3 expression between functional and silent corticotroph adenomas (Mann-Whitney U p value <0.001). The descriptive statistics and crosstabulation of Gal-3 expression are shown in Tables 1 & 2 . The distribution and bloxplot of comparison of Gal-3 expression are shown in Figures 4 and 5, respectively.
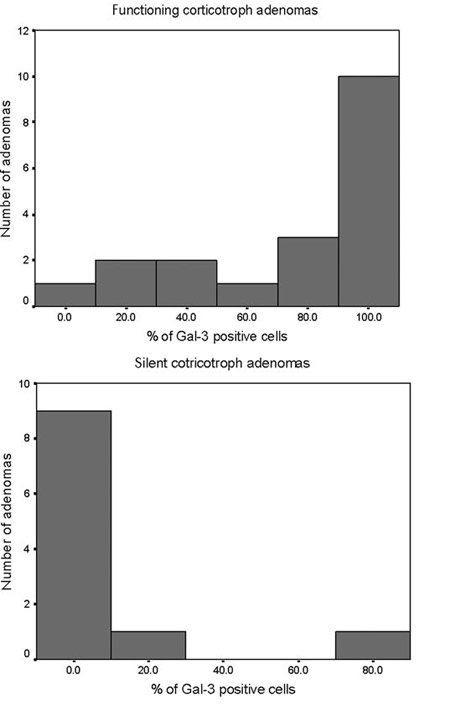
Figure 4. Distribution of expression of Gal-3 in functioning and silent corticotroph adenomas.
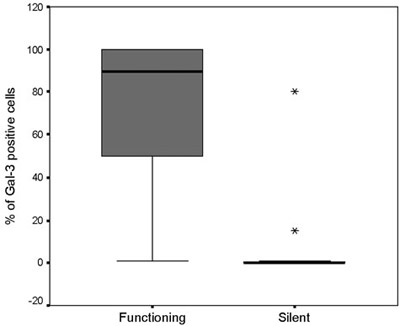
Figure 5. Boxplot of comparison of Gal-3 expression in functioning and silent corticotroph adenomas.
DISCUSSION
Silent corticotroph adenomas, first described by Horvath et al,14 are characterized by immunohistochemical staining of ACTH and other POMC derived peptides as β-endorphin; however, they are not associated with clinical signs of hypercortisolism. Two subtypes are described, subtype 1 and subtype 2, diagnosed only by electron microscopy. Clinically, they present as rapidly growing tumors causing symptoms related to their mass effect. Silent corticotroph adenomas are thought to derive from the basophilic POMC immunoreactive cells of the pars intermedia. These cells, which often invade the posterior lobe (basophilicinvasion), are identical with the functioning corticotroph cells of the pars distalis, with regard to their ultrastructural morphology basophilia in H&E stain, positivity via PAS technique, and immunoreactivity for ACTH and POMC derived peptides. Thus, silent corticotroph adenomas are histologically indistinguishable from the functioning ones, which are clinically associated either with Cushing’s disease or Nelson’s syndrome. Therefore, the differential diagnosis is based on clinical information alone. The only histological sign indicating that a corticotroph adenoma is silent is the absence of Crooke’s cells in the nontumorous corticotroph cells when adenohypophysial tissue fragments are included in the sample.12 Crooke’s hyaline changes represent deposits of cytokeratin intermediate filaments in the cytoplasm of corticotroph cells showing a characteristic glassy appearance. It is throught to represent a functioning response to the elevated serum cortisol levels, which is reversible. Reversibility of Crooke’s hyaline change after discontinuation of treatment with corticosteroids has been observed in autopsy studies.15
By electron microscopy, functioning and silent type 1 corticotroph adenomas show identical morphologic features, including the presence of cytokeratin intermediate filaments type 1, which represent their diagnostic hallmark. In contrast, silent type 2 adenomas are different and unlike, silent type 1 tumors, they are devoid of microfilaments type 1. Unfortunately, no other specific marker is available so far to differentiate the silent from the functioning subgroup of corticotroph adenomas.
A previous study of galectin mRNA by RT-PCR showed that galectins 1-9 were expressed in normal pituitary.11 Specifically, Gal-3, immunohistochemistry and western blot analysis revealed a differential pattern of expression in both normal and neoplastic pituitary; only lactotroph, corticotroph and folliculostellate cells as well as PRL and ACTH-producing tumors were positive. In addition, in normal pituitary, Gal-3 is detected in 5% of the corticotroph cells of the anterior lobe and in only a small subset, less than 1% in the corticotrophs invading the posterior lobe. More frequent expression of Gal-3 has also been reported, with variably diffuse immunopositivity, in 83% of functioning corticotroph adenomas from patients presenting with Cushing’s disease or Nelson’s syndrome, whereas focal expression was observed in only 20% of silent corticotroph adenomas.10,11 Our study further sustains these findings, since a substantial majority of functioning corticotroph adenomas expressed Gal-3, whereas only 2 of the silent corticotroph adenomas were Gal-3 positive. Considering the statistically significant difference in Gal-3 expression between the two groups of tumors, we suggest that Gal-3 can be applied as a useful marker in the diagnosis of silent corticotroph adenomas.
The reason for differing Gal-3 expression between silent and functioning corticotroph adenomas remains unclear. In a recent study investigating gonadotroph and null cell adenomas, the promoter region of the Gal-3 gene (LGALS3) was found to be methylated and silenced in a substantial number of tumors. In contrast, PRL-and ACTH-producing tumors, which were found unmethylated, expressed Gal-3 protein.16 Likewise, in silent corticotroph adenoma cells a probable methylation of LGALS3 may be an explanation for the absence of Gal-3. However, this suggestion remains to be documented.
p27-null mice produce mainly ACTH and develop pituitary hyperplasia and tumors of the intermediate lobe corticotroph cells. Gal-3 expression was found to be markedly increased in hyperplastic and neoplastic pituitaries from p27-null mice compared with control mice. Gal-3 was also found to be more frequently expressed in ACTH- producing pituitary carcinomas compared with adenomas. In addition, RNA interference experiments showed that Gal-3 has a direct stimulatory effect on cell growth and prevents apoptosis in cultured pituitary cells. All these observations suggest a direct role of Gal-3 in corticotroph cell tumorigenesis and tumor progression.10 With regard to our findings, the absence of Gal-3 expression in silent corticotroph adenomas indicates that Gal 3 may also interfere in the regulation of hormone production and release by corticotroph cells, a hypothesis to be examined. In conclusion, our results strongly suggest that Gal-3 immunostaining can be used as a specific marker in the pathologic diagnosis of silent ACTH-positive pituitary adenomas, particularly in cases where the clinical information is uncertain or unavailable.
REFERENCES
1. Barondes SH, Cooper DN, Gitt MA, Leffler H, 1994 Galectins: structure and function of a large family of animal lectins. J Biol Chem 269: 20807-20810.
2. Amado M, Almeida R, Schwientek T, Clausen H, 1999 Identification and characterization of large galactosyl-transferase gene families: galactosyltransferases for all functions. Biochem Biophys Acta 1473: 35-53.
3. Furukawa K, Sato T, 1999 β-1,4-Galactosylation of N-glycans is a complex process. Biochem Biophys Acta 1473: 54-66.
4. Inohara H, Akahani S, Koths K, Raz A, 1996 Interactions between galectin-3 and Mac-2-binding protein mediate cell-cell adhesion. Cancer Res 56: 4530-4534.
5. Nangia-Makker P, Honjo Y, Sarvis R, et al, 2000 Ga-lectin-3 induces endothelial cell morphogenesis and angiogenesis. Am J Pathol 156: 899-909.
6. Yoshii T, Fukumori T, Honjo Y, Inohara H, Kim HR, Raz A, 2002 Galectin-3 phosphorylation is required for its anti-apoptotic function and cell cycle arrest. J Biol Chem 277: 6852-6857.
7. Bresalier RS, Mazurek N, Sternberg LR, et al, 1998 Metastasis of human colon cancer is altered by modifying expression of the beta-galactoside-binding protein galectin-3. Gastroenterol 115: 287-296.
8. Xu XC, El-Naggar AK, Lotan R, 1995 Differential ex-pression of galectin-1 and galectin-3 in thyroid tumors. Potential diagnostic implications. Am J Pathol 147: 815-822.
9. Honjo Y, Nangia-Makker P, Inohara H, Raz A, 2001 Down regulation of galectin-3 supresses tumorigenicity of human breast carcinoma cells. Clin Cancer Res 7: 661-668.
10. Riss D, Jin L, Qian X, et al, 2003 Differential expression of galectin-3 in pituitary tumors. Cancer Res 63: 22512255.
11. Jin L, Riss D, Ruebel K, et al, 2005 Galectin-3 expression in functioning and silent ACTH-producing adenomas. Endocr Pathol 16: 107-114.
12. Mazarakis N, Kontogeorgos G, Kovacs K, Horvath E, Boroboli N, Piaditis G, 2001 Composite somatotroph -ACTH-immunoreactive pituitary adenoma with trans-formation of hyperplasia to adenoma. Pituitary 4: 215-221.
13. Trouillas J, Barkan AL, Watson RE Jr, Lindell EP, Far-rell WE, Lloyd RV 2004 ACTH producing adenoma. In: De Lellis RA, et al, (eds) WHO Classification of Tumours of the Endocrine Organs: Pathology and Genetics of Endocrine Organs, IARC Press, Lyon; pp, 26-29.
14. Horvath E, Kovacs K, Killinger DW, Smyth HS, Platts ME, Singer W, 1980 Silent corticotropic adenomas of the human pituitary gland. A histologic, immunocytologic, and ultra-structural study. Am J Pathol 98: 617-638.
15. Halmi NS, McCormick WF, Decker DA, 1971 The natural history of hyalinization of ACTH-MSH cells in man. Arch Pathol 91: 318-326.
16. Ruebel KH, Jin L, Qian X, et al, 2005 Effects of DNA methylation on galectin-3 expression in pituitary tumors. Cancer Res 65: 1136-1140.