HORMONES 2007, 6(3):218-226
DOI: 10.14310/horm.2002.——
Address for correspondence:
Dr. Ioannis Ilias, 129 Kifisias Avenue, Athens, 115 24, Greece, Fax: +30 210 6997507, e-mail: iiliasmd@yahoo.com
Received 05-03-07, Revised 06-06-07, Accepted 20-06-07
Abstract
OBJECTIVE: To evaluate whether tentative prognostic models for intensive care unit survival of multiple trauma patients could be improved by including endocrine parameters. DESIGN: Prospective study. Patients: Eighty-three male and 11 female multiple trauma patients. Measurements: Upon admission, severity of trauma was assessed with the Acute Physiology and Chronic Health Evaluation II (APACHE II), the Sequential Organ Failure Assessment (SOFA) score and the Injury Severity Score (IS). Concurrently, blood was drawn to measure thyrotropin (TSH), free thyroxine (fT4), trioodothyronine (T3), corticotropin (ACTH), prolactin (PRL), cortisol and dehydroepiandrosterone sulphate (DHEAS). Adrenal reserve was assessed with the Synacthen test. RESULTS: Seventy-five of the 83 men and 8 of the 11 women survived. APACHE II and SOFA scores were higher in non-survivors compared to survivors (with considerable overlap). From the baseline endocrine work-up, survivors had higher ACTH and DHEAS values compared to non-survivors (also with considerable overlap). No differences between survivors and non-survivors were noted in the Synacthen test or in thyroid function tests. Nevertheless, a multivariate logistic regression model that incorporated the APACHE II score and hormonal parameters (Cortisol post-Synacthen, DHEAS, TSH*age) was well-fitted to assess survival/non-survival as an endpoint and better than APACHE II, SOFA or IS scores alone to predict ICU survival or death. CONCLUSION: In critically ill multiple trauma patients, age, TSH, Cortisol post-Synacthen and DHEAS values upon admission to the ICU, combined with the APACHE II score, may predict outcome more accurately than the APACHE II score alone.an the APACHe II score alone.
Key words: Adrenal, Anterior pituitary hormones, Endocrine parameters, Intensive care unit, Logistic Models, Multiple trauma, ROC Curves, Thyroid
INTRODUCTION
The endocrine milieu of patients hospitalized in intensive care units (ICU) and/or in critical condition has been assessed in many studies1 and differences in pituitary, thyroid and adrenal function have been found between survivors and non-survivors.2 Nevertheless, an overlap of hormone values between patients in critical condition compared to controls or ICU survivors and non-survivors is generally noted in relevant studies. In a recent study of 206 patients, a logistic regression model incorporating a well-established clinical measure of ICU patients evaluation (the Acute Physiology and Chronic Health Evaluation II; APACHE II score), free triiodothyronine (fT3) and thyrotropin (TSH) values was shown to add to the prognostic value of APACHE II in patients with acute respiratory distress syndrome (ARDS).3 In the aforementioned study no patients with trauma were included. In another recent study of 113 ICU patients (with only 4 of them admitted because of trauma),the additionof TSH and total T3 improved the prognostic value of the APACHEII score.4 An older study of260 ICU patients (with only 5 of them admitted because of trauma) showed that the combination of TSH, thyroxine (T4) and cortisol was a better predictor of survival than the APACHE II score.2 Interestingly, TSH values in earlier studies of fewer ICU patients with trauma were mostly low5 or suppressed6 but were not associated with survival.7,8 Among other endocrine parameters, “occult” or frank adrenal insufficiency9 has been linked in some studies with an adverse outcome of patients with trauma,10 but not in others.11,12 The aim of the present study was to evaluate whether or not prediction of outcome in ICU patients with trauma could be improved by combining clinical assessment models with parameters of pituitary, thyroid and adrenal function.
SUBJECTS AND METHODS
Subjects
This was a prospective study of 83 male and 11 female (age [mean±sd] 35.8±16.6 years) trauma patients (63 with head trauma) hospitalized at a single tertiary-care teaching hospital’s ICU from August 2003 to December 2005. Gender was taken into consideration as an independent dichotomous variable in statistical analysis. Exclusion criteria included prior (within the past year) use of corticosteroids, concurrent treatment with drugs affecting the hypothalamic-pituitary activity (etomidate, diphenyl-hydantoin or rifampicin) and a known pre-existing endocrine disorder. The hospital’s ethics committee gave their approval for the performance of the study. Informed consent was obtained from the patients’ next of kin.
Treatment
The administration of dopamine (shown to inhibit pituitary hormone secretion and in particular prolactin (PRL)13,14 or TSH in most,15-17 but not all,18 clinical studies) to patients was recorded and was taken into consideration as an independent dichotomous variable in statistical analysis.
Measures
Upon admission in the ICU, severity of trauma was assessed by means of APACHE II, Sequential Organ Failure Assessment (SOFA) score and Injury Severity Score (ISS). Concurrently, blood was drawn to measure TSH, free T4 (fT4), T3, corticotropin (ACTH), PRL, cortisol and dehydroepiandrosterone sulphate (DHEAS). Furthermore, to assess adrenal reserve, cortisol was measured 30 minutes after the intravenous administration of 1 microgram of synthetic ACTH (Cosyntropin; Synacthen test) (Synacthène, Novartis, Basel, Switzerland). The choice of the 1 microgram Synacthen test over the 250 microgram was based on published studies showing that the higher dose is supraphysiologic and may miss mild cases of adrenal insufficiency.19,20 Furthermore, the 1 microgram Synacthen test has already been validated in ICU patients.12,21
Assays
Commercial assays were used for measurement of endocrine parameters: TSH, fT4 and T3 with electrochemiluminescence (Elecsys Systems, Roche Diagnostics, Mannheim, Germany), ACTH with an immunoradiometric assay (Nichols Institute Diagnostics, San Juan Capistrano, CA, USA), PRL with chemiluminescence (Bayer Corporation, NY, USA), cortisol with an immunofluorometric assay (Chiron Corporation, East Walpole, MA, USA) and DHEAS with a radioimmunoassay (Coat-A-Count, Diagnostic Products Corporation, CA, USA).
Statistical analysis
Values of quantitative parameters that were either calculated (APACHE II, SOFA, ISS) or measured (all the endocrine function values) are presented as means + SD, as well as median and range. Normality of distribution was assessed with Wilks-Shapiro’s test. Qualitative measures (gender, presence of head trauma) are presented according to survival. Comparisons of quantitative parameters between survivors/non-survivors were made with unpaired Student’s t-tests and Wilcoxon’s test (if their distribution was not normal). Comparisons of qualitative parameters between survivors/non-survivors were made with Fisher’s exact test. Univariate logistic regression models of all the observed, calculated and measured parameters with survival/non-survival as the dependent variable were separately created. Multivariate logistic regression models were then created, using the same variables as in univariate logistic regression analysis plus composite variables (from acorrelation matrix).22 Models were sequentially selected by a backwards stepwise process based on the likelihood ratio of survival/non-survival. Further selection of the models obtained was based on the Hosmer-Lemeshow chi-square goodness-of-fit criterion (according to this criterion, the better suited models have lower chi-square values and higher p probability values).23 Finally, the predictive power of the univariate logistic regression models and of the selected multivariate models was assessed with receiver operating characteristic (ROC) plots; comparisons of ROCs were made based on their area under the curve (AUC).24
RESULTS
Seventy-five of the 83 men and 8 of the 11 women survived and were transferred to medical or surgical hospital wards. Thirteen patients (11 survivors and 2 non-survivors) received dopamine infusion.
The APACHE II and SOFA scores were higher in non-survivors compared to survivors (Table 1 ). The overlap of these clinical severity scores was considerable between survivors and non-survivors. From the baseline endocrine evaluation, we found that survivors had higher PRL and DHEAS levels compared to non-survivors (Table 2 ). As with the clinical severity scores, the overlap between survivors and non-survivors was considerable. No significant differences between survivors and non-survivors were noted in the Synacthen or thyroid function tests. The presence of head trauma or dopamine administration was not significantly correlated with any of the hormonal parameters, whereas age was correlated with hormone levels (data not shown for simplicity; see below for further analysis of parameters with age).
The univariate logistic regression results were concordant with the comparisons carried out with the Student’s, Wilcoxon’s and Fisher’s tests (Table 1). APACHE II, SOFA, ISS scores or DHEAS levels alone predicted ICU patients survival or death correctly in 85, 84, 83 and 84 of 94 cases, respectively. ROC plot analysis showed that, among the univariate parameters, the clinical severity scores and DHEAS were the most predictive (either with AUC of the ROC or the upper 95% CI of the ROC larger than 0.80). Among the many multivariate logistic regression models that were created, one that incorporated the APACHEII score and hormonal parameters (DHEAS and TSH*age) was well-fitted to assess survival/non-survival as an endpoint (with the Hosmer-Lemeshow chi-square goodness -of-fit criterion) (Table3 ).Specifically, DHEAS and TSH*age contributed negatively to the logit probability of ICU death. This multivariate logistic regression model correctly predicted ICU survival or death correctly in 85 of 94 cases (as many as with the APACHE score alone). However, the corresponding ROC plot for this multivariate model had a much higher AUC compared to the AUCs of the ROCs obtained for APACHE II, SOFA or ISS scores alone. Consequently, this multivariate model was a better predictor of survival or death compared to APACHE II, SOFA or ISS scores alone (Table 3 and Figure 1).
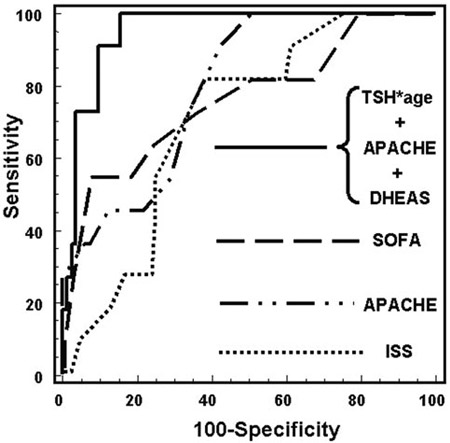
Figure 1. ROC plots for the final multivariate logistic regression model vs APACHE II, ISS and SOFA ROCs.
DISCUSSION
In this study of patients with trauma, survival prediction was better by combining the APACHE II score with age, TSH and DHEAS values than with the APACHE II score alone.
The mechanisms of endocrine changes in patients with trauma are not well known. For those with head trauma, anatomical abnormalities (vascular insult in the hypothalamic-pituitary area or basal skull fractures)25 or functional alterations related to brain edema, elevated intracranial pressure,5,26 hypotensive and/or hypoxic insults27 and cytokines, in particular interleukin-6,28 have all been implicated.
Prolactin rises in the acute phase of critical illness; this rise has been attributed to the actions of vasoactive intestinal polypeptide, oxytocin or cytokines.29 Higher PRL has been noted in trauma patients compared to other ICU patients.5,30 In our study PRL was not included in the final predictive model; however, we found higher PRL levels in survivors compared to non-survivors. The possible association between PRL and survival and the mechanism involved warrants further investigation.31-35
Regarding the pituitary-thyroid axis, conflicting results have been presented vis-à-vis survival in patients in critical condition.36 In some studies, low or high TSH and low T3 or low T4 have been associated with higher mortality,37-41 while other studies have not found any such association.42,43 Moreover, in a study of multiple trauma patients, low T4 was associated with higher mortality.40 In our study overall thyroid function was within normal limits; however, the factor of TSH*age was negatively associated with mortality. This may possibly indicate that the condition of these patients is improving, since it is known that in critically ill patients a high TSH is an indication of recovery from “non-thyroidal illness” (“euthyroid sick syndrome”).44,45
Cortisol rises in trauma and/or sepsis, probably to counteract the inflammatory cytokine response to such conditions.46 Studies examining the prognostic value of baseline and Synachten-stimulated serum cortisol in critically ill patients have failed to demonstrate a reproducible correlation between cortisol responses and outcome.9 Both high and low cortisol levels have been associated with higher mortality, whereas others showed that cortisol levels failed to predict clinical outcome.9 In our patients with multiple trauma, neither pre- or post-Synacthen cortisol nor Δcortisol levels contributed to the final (best) logistic regression model. These parameters were removed according to the likelihood ratio-based backwards stepwise process and the Hosmer-Lemeshow chi-square goodness-of-fit criterion (detailed data were not shown in the results section for simplicity).
The profile of DHEAS has not been studied as extensively as that of cortisol in critical illness.9 In certain studies DHEAS was found to be lower in ICU patients compared to healthy individuals;10,47 this has been attributed to a shift of steroidogenesis to cortisol production by critical illness.48 Significantly higher DHEAS levels were noted in our trauma survivors than in non-survivors and DHEAS was included in the logistic regression model. The association of high DHEAS with lower mortality found in our study might be explained by its immunoenhancing properties, since it has been shown that DHEA, the most plentiful steroid hormone, activates the monocyte-macrophage system, antagonizes the suppressive effects of dexamethasone on lymphocyte proliferation, exerts a direct immunostimulatory effect on murine T cells and increases cytokine production. Nevertheless, the relevant clinical findings are considered to be controversial.9,10,48-52
The number of patients who did not survive in our study was relatively small and this constitutes a limitation. This could also explain the lack of statistical significance in the other hormone levels between survivors and non-survivors. Clearly, further investigation in a larger cohort is needed to better define endocrine predictors in polytraumatized, critically ill patients in order to assess the utility – if any – of such predictors in the clinical management of these patients.
In conclusion, in critically ill patients with trauma, age, TSH and DHEAS levels upon admission to the ICU, in combination with the APACHE II score, may predict outcome more accurately than the APACHE II score alone.
REFERENCES
1. Van den Berghe G, 2003 Endocrine evaluation of patients with critical illness. Endocrinol Metab Clin North Am 32: 385-410.
2. Rothwell PM, Lawler PG, 1995 Prediction of outcome in intensive care patients using endocrine parameters. Crit Care Med 23: 78-83.
3. Ture M, Memis D, Kurt I, Pamukcu Z, 2005 Predictive value of thyroid hormones on the first day in adult respiratory distress syndrome patients admitted to ICU: comparison with SOFA and APACHE II scores. Ann Saudi Med 25: 466-472.
4. Chinga-Alayo E, Villena J, Evans AT, Zimic M, 2005 Thyroid hormone levels improve the prediction of mor-tality among patients admitted to the intensive care unit. Intensive Care Med 31: 1356-1361.
5. Chiolero R, Lemarchand T, Schutz Y, et al, 1988 Plasma pituitary hormone levels in severe trauma with or without head injury. J Trauma 28: 1368-1374.
6. Schilling JU, Zimmermann T, Albrecht S, Zwipp H, Saeger HD, 1999 Low-T3-Syndrom bei Polytrauma patienten—Phänomen oder wichtiger pathogenetischer Faktor? Med Klin (Munich) 94: Suppl 3: 66-69.
7. Mocchegiani E, Imberti R, Testasecca D, Zandri M, Santarelli L, Fabris N, 1995 Thyroid and thymic endocrine function and survival in severely traumatized patients with or without head injury. Intensive Care Med 21: 334-341.
8. Hackl JM, Gottardis M, Wieser C, et al, 1991 Endocrine abnormalities in severe traumatic brain injury–a cue to prognosis in severe craniocerebral trauma? Intensive Care Med 17: 25-29.
9. Arafah BM, 2006 Hypothalamic Pituitary Adrenal Function During Critical Illness: Limitations of Current Assessment Methods. J Clin Endocrinol Metab 91: 3725-3745.
10. Beishuizen A, Thijs LG, Vermes I, 2002 Decreased levels of dehydroepiandrosterone sulphate in severe critical illness: a sign of exhausted adrenal reserve? Crit Care 6: 434-438.
11. Gannon TA, Britt RC, Weireter LJ, Cole FJ, Collins JN, Britt LD, 2006 Adrenal insufficiency in the critically III trauma population. Am Surg 72: 373-376.
12. Dimopoulou I, Tsagarakis S, Douka E, et al, 2004 The low-dose corticotrophin stimulation test in acute traumatic and non-traumatic brain injury: incidence of hypo-responsiveness and relationship to outcome. Intensive Care Med 30: 1216-1219.
13. Bailey AR, Burchett KR, 1997 Effect of low-dose dopamine on serum concentrations of prolactin in critically ill patients. Br J Anaesth 78: 97-99.
14. Serri O, Kuchel O, Buu NT, Somma M, 1983 Differential effects of a low dose dopamine infusion on prolactin secretion in normal and hyperprolactinemic subjects. J Clin Endocrinol Metab 56: 255-259.
15. Kaptein EM, Spencer CA, Kamiel MB, Nicoloff JT, 1980 Prolonged dopamine administration and thyroid hormone economy in normal and critically ill subjects. J Clin Endocrinol Metab 51: 387-393.
16. Rabey JM, Vardi Y, Ravid R, Ayalon D, 1981 Dissociation of thyrotropin and prolactin responsiveness to thyrotropin releasing hormone stimulation in L-dopa treated parkinsonian patients. Horm Res 15: 78-87.
17. Boesgaard S, Hagen C, Hangaard J, Andersen AN, El-drup E, 1990 Effect of dopamine and a dopamine D-1 receptor agonist on pulsatile thyrotrophin secretion in normal women. Clin Endocrinol (Oxf) 32: 423-431.
18. Connell JM, Ball SG, Inglis GC, Beastall GH, Davies DL, 1984 The effect of low-dose dopamine infusion on anterior pituitary hormone secretion in normal female subjects. Clin Sci (Lond) 67: 219-223.
19. Angele MK, Catania RA, Ayala A, Cioffi WG, Bland KI, Chaudry IH, 1998 Dehydroepiandrosterone: an inexpensive steroid hormone that decreases the mortality due to sepsis following trauma-induced hemorrhage. Arch Surg 133: 1281-1288.
20. Kozyra EF, Wax RS, Burry LD, 2005 Can 1 microg of cosyntropin be used to evaluate adrenal insufficiency in critically ill patients? Ann Pharmacother 39: 691-698.
21. Sarthi M, Lodha R, Vivekanandhan S, Arora NK, 2007 Adrenal status in children with septic shock using low-dose stimulation test. Pediatr Crit Care Med 8: 23-28.
22. Hosmer DW, Lemeshow S 2000 Model-building strategies and methods for logistic regression. In: Hosmer DW, Lemeshow S (ed) Applied logistic regression New York, John Wiley & Sons; pp, 91-142.
23. Hosmer DW, Lemeshow S 2000 Assessing the fit of the model .In: Hosmer DW, Lemeshow S (ed) Applied logistic regression New York: John Wiley & Sons; pp, 143-202.
24. Hanley JA, McNeil BJ, 1983 A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology 148: 839-843.
25. Bondanelli M, Ambrosio MR, Zatelli MC, De Marinis L, Uberti EC, 2005 Hypopituitarism after traumatic brain injury. Eur J Endocrinol 152: 679-691.
26. Feibel J, Kelly M, Lee L, Woolf P, 1983 Loss of adrenocortical suppression after acute brain injury: role of increased intracranial pressure and brain stem function. J Clin Endocrinol Metab 57: 1245-1250.
27. Kelly DF, Gaw Gonzalo IT, Cohan P, Berman N, Swerdloff R, Wang C, 2000 Hypopituitarism following traumatic brain injury and aneurysmal subarachnoid hemorrhage: a preliminary report. J Neurosurg 93: 743-752.
28. Dimopoulou I, Tsagarakis S, Kouyialis AT, et al, 2004 Hypothalamic-pituitary-adrenal axis dysfunction in critically ill patients with traumatic brain injury: Incidence, pathophysiology, and relationship to vasopressor dependence and peripheral interleukin-6 levels. Crit Care Med 32: 404-408.
29. Van den Berghe G, 2000 Novel insights into the neuro-endocrinology of critical illness. Eur J Endocrinol 143: 1-13.
30. Lindh A, Carlstrom K, Eklund J, Wilking N, 1992 Serum steroids and prolactin during and after major surgical trauma. Acta Anesthesiol Scand 36: 119-124.
31. Russell DH, 1989 New aspects of prolactin and immunity: a lymphocyte-derived prolactin-like product and nuclear protein kinase C activation. Trends Pharmacol Sci 10: 40-44.
32. Vanhorebeek I, Van den Berghe G, 2006 The neuroen-docrine response to critical illness is a dynamic process. Crit Care Clin 22: 1-15.
33. Dimopoulou I, Tsagarakis S, Theodorakopoulou M, et al, 2004 Endocrine abnormalities in critical care patients with moderate-to-severe head trauma: incidence, pattern and predisposing factors. Intensive Care Med 30: 1051-1057.
34. Dorshkind K, Horseman ND, 2001 Anterior pituitary hormones, stress, and immune system homeostasis. Bioessays 23: 288-294.
35. Van den Berghe G, de Zegher F, Bouillon R, 1998 Acute and prolonged critical illness as different neuroendocrine paradigms. J Clin Endocrinol Metab 83: 1827-1834.
36. Sesmilo G, Halperin I, Puig-Domingo M, 2007 Endocrine evaluation of patients after brain injury: what else is needed to define specific clinical recommendations. Hormones (Athens) 6: 132-137.
37. Rothwell PM, Udwadia ZF, Lawler PG, 1993 Thyrotropin concentration predicts outcome in critical illness. Anaesthesia 48: 373-376.
38. Jarek MJ, Legare EJ, McDermott MT, Merenich JA, Kollef MH, 1993 Endocrine profiles for outcome prediction from the intensive care unit. Crit Care Med 21: 543-550.
39. Maldonado LS, Murata GH, Hershman JM, Braunstein GD, 1992 Do thyroid function tests independently predict survival in the critically ill? Thyroid 2: 119-123.
40. Kaptein EM, Weiner JM, Robinson WJ, Wheeler WS, Nicoloff JT, 1982 Relationship of altered thyroid hormone indices to survival in nonthyroidal illnesses. Clin Endocrinol (Oxf) 16: 565-574.
41. Arem R, Thornby JI, Deppe SA, 1997 Comparison of thyroid hormone and cortisol measurements with Apache II and TISS scoring systems as predictors of mortality in the medical intensive care unit. J Intens Care Med 12: 12-17.
42. Ray DC, Drummond GB, Wilkinson E, Beckett GJ, 1995 Relationship of admission thyroid function tests to outcome in critical illness. Anaesthesia 50: 1022-1025.
43. Gottardis M, Luger TJ, Benzer A, Fridrich L, 1993 Evaluation of thyroid hormones as predictor of outcome in patients after major trauma. Thyroid 3: 355-356.
44. Utiger RD 2001 The thyroid: physiology, thyrotoxicosis, hypothyroidism and the painful thyroid. In: Felig P, Frohman LA (ed) Endocrinology & Metabolism New York: McGraw-Hill; pp, 261-347.
45. Spencer C, Eigen A, Shen D, et al, 1987 Specificity of sensitive assays of thyrotropin (TSH) used to screen for thyroid disease in hospitalized patients. Clin Chem 33: 1391-1396.
46. Annane D, 2001 Corticosteroids for septic shock. Crit Care Med 29: S117-S120.
47. Wade CE, Lindberg JS, Cockrell JL, et al, 1988 Upon-admission adrenal steroidogenesis is adapted to the degree of illness in intensive care unit patients. J Clin Endocrinol Metab 67: 223-227.
48. Dhatariya KK, 2003 Is there a role for dehydroepiandrosterone replacement in the intensive care population? Intensive Care Med 29: 1877-1880.
49. Chen CC, Parker CRJ, 2004 Adrenal androgens and the immune system. Semin Reprod Med 22: 369-377.
50. Oberbeck R, 2004 Therapeutic implications of immune-endocrine interactions in the critically ill patients. Curr Drug Targets Immune Endocr Metabol Disord 4: 129-139.
51. Marx C, Petros S, Bornstein SR, et al, 2003 Adrenocortical hormones in survivors and nonsurvivors of severe sepsis: diverse time course of dehydroepiandrosterone, dehydroepiandrosterone-sulfate, and cortisol. Crit Care Med 31: 1382-1388.
52. Folan MM, Stone RA, Pittenger AL, Stoffel JA, Hess MM, Kroboth PD, 2001 Dehydroepiandrosterone, dehy-droepiandrosterone-sulfate, and cortisol concentrations in intensive care unit patients. Crit Care Med 29: 965-970.