HORMONES 2006, 5(4):303-309
DOI: 10.14310/horm.2002.——
Address correspondence and requests for reprints to:
Evangeline Vassilatou MD, PhD, “Amalia Fleming” General Hospital, Department of Endocrinology, Diabetes and Metabolism, 14 25th March Str., GR-151 27 Melissia, Athens, Greece, Tel: +30 210 8038294, Fax: +30 210 8047656, e-mail: niadas@hol.gr
Received 04-07-06, Revised 20-08-06, Accepted 25-08-06
Abstract
Thyroid tumors producing colony-stimulating factors associated with neutrophilia and/or eosinophilia are very rare and almost all of them concern anaplastic thyroid cancer. Only one case of papillary thyroid carcinoma associated with neutrophilia and one case of medullary thyroid carcinoma associated with eosinophilia have been reported. In this report a 72-year old male patient with metastatic papillary thyroid carcinoma associated with neutrophilia and eosinophilia is described. While investigating the cause of neutrophilia and eosinophilia, a blind bone marrow biopsy of the posterior iliac crest was performed, which showed infiltration by papillary thyroid carcinoma. High blood levels of granulocyte-macrophage colony-stimulating factor (GM-csF) were found using an enzyme-linked immunosorbent assay. As other causes of neutrophilia and eosinophilia were excluded, we assumed that these were paraneoplastic manifestations induced by GM-csF produced by the thyroid tumor. the disease progressed rapidly, despite appropriate treatment which included thyroidectomy and postoperative radioactive 131I administration. the patient died 11 months after diagnosis because of extensive lung metastasis. Neutrophilia and eosinophilia were stable findings, while serum thyroglobulin levels remained elevated throughout the follow-up period. to our knowledge, this is the first report of a patient with metastatic papillary thyroid carcinoma in whom neutrophilia and eosinophilia associated with high circulating levels of GM-csF were detected.
Key words: Eosinophilia, Neutrophilia, GM-CSF, Thyroid cancer
INTRODUCTION
Marked neutrophilia and/or eosinophilia associated with neoplasia are relatively rare findings and have been considered as paraneoplastic manifestations after excluding other causes, such as infections, allergy, collagen disease, vascular diseases, and concomitant
malignant haematopoietic diseases.1 Production of haematopoietic growth factors by the tumor has been reported in some patients with neutrophilia and/or eosinophilia in the context of non-lymphohematopoietic malignancies, most often lung cancer.2-8 This ectopic production is also supported by in vitro data showing secretion of colony-stimulating factors by tumor cell lines.9,10 Colony-stimulating factors are thought to be the cause of the observed neutrophilia and/or eosinophilia, although the mechanism of induction has not been clarified.
Thyroid tumors producing colony-stimulating factors and associated with neutrophilia and/or eosinophilia have been described almost exclusively in patients with anaplastic thyroid cancer.11-17 Only two patients with differentiated thyroid cancer have thus far been reported, one with papillary type associated with neutrophilia18 and one with medullary type associated with eosinophilia.19
We report a patient with metastatic thyroid papillary carcinoma, in whom marked neutrophilia and eosinophilia and high circulating levels of GM-CSF were detected. We assume that this haematopoietic growth factor was produced by the tumor and caused the observed neutrophilia and eosinophilia.
PATIENT DESCRIPTION
In September 2003 a 72-year old male patient presented to his general practitioner with haemoptysis, general fatigue, and weakness. His chest X-ray showed bilateral nodular lesions. His past medical history included hypertension for the past three years, treated with enalapril 5mg/day and amlodipine 5mg/day, benign prostatic hyperplasia treated for the past two years with tamsulosin 0.4mg/day, and a serious bout of pneumonia at the age of 25. He had stopped smoking 12 years previously, but till then had been a heavy smoker (2-3 packets/day). As for his family history, his father died of liver cancer.
On November 4, 2003 the patient was admitted to our hospital for evaluation of lung lesions. Physical examination did not reveal any abnormal findings. Laboratory tests showed a mild leukocytosis with neutrophilia and eosinophilia, normal red blood cell and platelet count, and an increased erythrocyte sedimentation rate (Table 1 ). It has to be noted that 7 months earlier (April 2003), eosinophilia was detected while white blood cell count was normal (WBC: 10900/l with 66% neutrophils, 23% lymphocytes and 8% eosinophils). All other laboratory parameters were normal. A computed tomography of the chest showed multiple bilateral macro- and micronodular infiltrates and mediastinal lymphadenopathy. An extensive investigation followed; fibre optic bronchoscopy and bronchoalveolar lavage, laboratory testing for common infections, tuberculosis, and sarcoidosis. Bone scintigraphy with technetium pertechnetate 99, and abdomen and brain computed tomography revealed no abnormal findings. An open lung biopsy was performed and a specimen from the upper left lobe was excised, measuring 3.5×3.0x1.8cm. Histology showed the presence of metastatic papillary thyroid carcinoma, confirmed by positive immunohistochemical staining for thyroglobulin and TTF1 (thyroid transcription factor 1).
A thyroid investigation followed which showed normal levels of TSH and thyroid hormones, negative antithyroid antibodies, and normal levels of calcitonin. Serum thyroglobulin was 2476ng/ml (2476g/l) (Table 2 ). Neck ultrasonography showed a slight increase of the size of the right thyroid lobe and the presence of two hypoechogenic nodules, the bigger in the lower pole of the right lobe measuring approximately 1.0cm. A thyroid scan with technetium pertechnetate 99 showed the presence of a cold nodule in the lower pole of the right lobe. Fine needle aspiration was performed and cytology disclosed papillary thyroid carcinoma. The patient underwent thyroidectomy on December 16, 2003. The removed thyroid gland weighed ~20gr and on sections of the gland, a neoplastic lesion of 1.0cm was found in the periphery of the right lobe. Histology showed the presence of papillary thyroid carcinoma, tall cell variant, with abundant psammoma bodies in the tumor stroma, and no invasion of the thyroid capsule.
Three weeks after surgery (January 2004), the patient was admitted to the Endocrinology Department for postoperative evaluation and treatment. His symptoms had worsened, although haemoptysis did not recur, and he had developed low-grade fever. On physical examination there were no abnormal findings. Laboratory evaluation showed a worsening of neutrophilia and eosinophilia (Figure 1). No blasts were detected in peripheral blood. Red blood cell and platelet count were normal, as before. Serum thyroid stimulating hormone was elevated [32.1U/ml (32.1mU/l)] and triiodothyronine and free thyroxine were reduced [0.64ng/ml (0.98nmol/l) and 0.27ng/ dl (3.48pmol/l), respectively]. Serum thyroglobulin was 2143ng/ml (2143g/l) with negative thyroglobulin antibodies. Technetium pertechnetate 99 scan showed thyroid remnants in the upper part of the right thyroid bed. No lesions were depicted in bone X-rays. One week after admission, a dose of 70mCi of iodine 131 was administered to the patient for ablation of thyroid remnants. A post-therapy total body scan (I131– TBS) was performed four days after ablation treatment, which showed foci of uptake in the thyroid bed and probably in the upper mediastinum. The patient then received a TSH-suppression therapy with triiodothyronine (75μg/24h) with the prospect of a new treatment with iodine 131 for his metastatic disease.
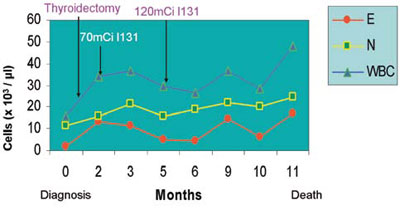
Figure 1. Variation in the number of neutrophils (N), eosinophils (E) and white blood cells (WBC) during disease course. Therapeutic interventions did not affect neutrophilia and eosinophilia.
The patient was subsequently referred to the Haematology department. In February 2004, he had a thorough investigation for common infections, parasitic, allergic, collagen-vascular, and skin diseases which can be associated with neutrophilia and eosinophilia, without any abnormal finding. Furthermore, as the administration of antibiotics for a short time did not affect the haematologic abnormalities and his low-grade fever persisted, a trial treatment of isoniazid and rifampicin was started because mycobacterial tuberculosis was highly suspected. to elucidate the cause of neutrophilia and eosinophilia, a blind bone marrow biopsy of the posterior iliac crest was performed. Smear analysis disclosed increased cellularity, significant increase of eosinophils, mostly of mature forms, absence of increased number of marrow blast cells and dysplasia, infiltration by plasma cells in 8% of the nucleated marrow cells,andnormal erythroid and megakaryocytic lineages. Histology showed infiltration by papillary thyroid carcinoma, confirmed by positive immunohistochemical staining for thyroglobulin (Figure 2), while staining for synaptophysin, chromogranin, and carcinoembryonic antigen (CEA) was negative. Cytogenetic examination of bone marrow cells, in order to exclude clonality, showed a normal karyotype. No BCR-ABL positivity was detected in peripheral blood neutrophils. For further investigation of neutrophilia and eosinophilia, serum concentrations of granulocyte colony-stimulating factor (G-CSF), granulocyte-macrophage colony-stimulating factor (GM-CSF), interleukin-3 (IL-3), interleukin-5 (IL-5), and tumor necrosis factor alpha (TNF-) were measured by an enzyme-linked immunosorbent assay (Quantikine, R&D Systems, Inc, Minneapolis, USA). Intra- and interassay coefficients of variation were less than 6% and sensitivity was 3.0pg/ml. Serum levels of granulocyte-macrophage colony-stimulating factor (GM-CSF) were 267.4pg/ml (2.22IU/ml) (normalless than 7.8pg/ml), whereas levels of G-CSF, IL-3, IL-5 and TNF- were within the normal range (Table 3 ). Anti-TBC treatment was then discontinued.
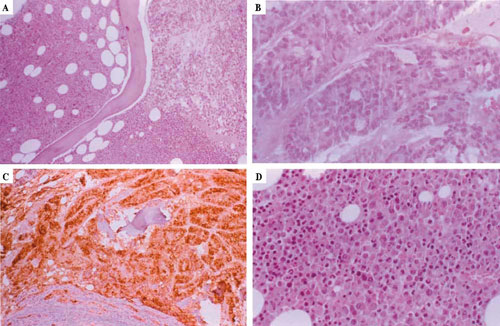
Figure 2. Histology sections of bone marrow biopsy of posterior iliac crest. A) Infiltration by papillary thyroid carcinoma (x100 H/E). B) Metastatic carcinoma with a predominantly follicular architecture (x400 H/E). C) Positive Tg immunostaining (x100). D) Functional bone marrow with eosinophilic hyperplasia (x400 H/E).
In April 2004, the patient’s fatigue and weakness worsened. Laboratory evaluation showed small changes in neutrophilia and eosinophilia (Figure 1), anaemia (red blood cell count: 4.38×106, haematocrit: 36.4%), and a normal platelet count. Serum thyroglobulin levels were greater than 1000ng/ml (>1000g/l) under triiodothyronine suppressive therapy. His chest X-ray showed an increase in the number and size of lung metastases and a worsening of mediastinal lymphadenopathy. The patient was hospitalised again and, after appropriate discontinuation of triiodothyronine regimen, he received a dose of 120mCi of iodine 131. A second post-therapy total body scan (I131-TBS) was performed, which still showed foci of uptake in the thyroid bed but no uptake by the lung metastatic lesions. This time he received a thyroxine suppressive therapy.
In May 2004, bone metastatic lesions (in the paravertebral part of the left 8th rib, in the front part of the left 6th rib, in the right sacroiliac joint, the right acetabulum, and a suspicious finding in the middle part of the sacrum) were shown in a second bone scintigraphy with technetium pertechnetate 99. Laboratory evaluation showed a small reduction of neutrophilia and eosinophilia (Figure 1), a worsening of anaemia, and a normal platelet count. Serum thyroglobulin levels were greater than 1000ng/ml (>1000g/l) under thyroxine suppressive therapy.
The patient’s clinical condition gradually worsened. Short courses of prednisone were administered, with a small improvement after the first three courses but without effect thereafter. As lung metastatic lesions progressed, he developed respiratory failure and died on October 7, 2004. An autopsy was not performed. Laboratory evaluation a few days before his death showed a worsening of neutrophilia and eosinophilia (Figure 1), anaemia, and the presence of thrombocytopenia (91×103/l).
DISCUSSION
The patient herein presented had a combination of very interesting findings that have not so far been described: a metastatic papillary thyroid carcinoma associated with both neutrophilia and eosinophilia and high circulating levels of GM-CSF.
Few patients with thyroid tumors and paraneoplastic leukocytosis have been reported since the first published case in 1954.20 In all described cases, metastatic disease was present when paraneoplastic leukocytosis was detected, as in our patient. Almost all cases concern anaplastic thyroid cancer with only two reported cases with differentiated thyroid carcinoma; one with papillary thyroid carcinoma associated with neutrophilia18 and one with medullary thyroid carcinoma associated with eosinophilia.19 In the patient we present, histology of the primary lesion showed tall cell variant of papillary thyroid cancer. Papillary thyroid carcinoma was also found in lung lesions and in bone marrow aspirate. Anaplastic transformation of this papillary thyroid carcinoma at the terminal stage of the disease is highly improbable based on clinical, biochemical, and histological data. At diagnosis, the primary tumor was small (1.0cm in diameter), confined in the thyroid gland, although metastatic disease was present. In contrast, patients with anaplastic transformation of a differentiated thyroid tumour usually present with a rapidly enlarging neck mass accompanied by compressive symptoms, due to invasion of adjacent organs. Serum thyroglobulin levels remained very high throughout the course of the disease and there was positive immunohistochemical staining for thyroglobulin in primary tumor and metastatic tissue. No invasion of the thyroid capsule was observed and no anaplastic foci were detected in any of the lesions examined.
Most of the reported patients with thyroid tumors and paraneoplastic leukocytosis had neutrophilia,11-14,17 few had eosinophilia,19-22 and only one had both neutrophilia and eosinophilia,15 as the patient we describe. Production of colony-stimulating factors, such as G-CSF,13-15 GM-CSF15,16 and M-CSF17 by the tumor, has been related to paraneoplastic leukocytosis, although the mechanism of induction of this haematologic abnormality remains unknown. High circulating levels of colony-stimulating factors in combination with either high concentrations of these factors in primary tumor and metastatic lesions15 or positive immunostaining for these factors in tumor tissue have confirmed this ectopic production.7,13 Moreover, production of colony-stimulating factors by thyroid cancer cell lines, mostly of the anaplastic type, has been demonstrated in some studies.9,23,24 Asakawa et al24 showed the secretion of G-CSF in one out of two poorly differentiated thyroid cancer cell lines examined, while no G-CSF secretion was detected in a papillary thyroid cancer cell line. The ability to produce colony-stimulating factors is not restricted to malignant thyroid cells, as studies of thyroid epithelial cells from patients with Graves’ disease and non-toxic goiter have shown25,26 colony stimulating factor production. The pathophysiological significance of colony-stimulating factor production by thyroid epithelial cells is unclear. It is known that growth factors exert most of their effects locally, so it may be suggested that the above findings reflect autocrine or paracrine actions in the thyroidal microenvironment. Under certain conditions, this production may be up-regulated in thyroid cancer cells, resulting in the release of large amounts of colony-stimulating factors in the circulation causing leukocytosis in the late stage of the disease. Data from animal models support the notion of an oncogene-induced cytokine secretion, which is important for the development and progression of thyroid cancer in genetically permissive hosts.27
Human GM-CSF is a N-glycosylated polypeptide of 127 aminoacids and a potent activator of proliferation and differentiation of myeloid stem cells to neutrophils, eosinophils, and monocytes/macrophages.28 These actions can explain the appearance of both neutrophilia and eosinophilia in patients with tumors producing GM-CSF, as previously described5,15 as well as in the present case. Paraneoplastic neutrophilia without eosinophilia has also been reported in a patient with increased circulating levels of GM-CSF.12 GM-CSF production by thyroid cancer, either isolated16 or in combination with other cytokines15 seems to be a very rare finding, as only three cases have been reported.12,15,16 In the case described by Murabe et al,12 high circulating levels of GM-CSF were detected, although the authors do not comment on whether other colony-stimulating factors were evaluated. It has to be noted that these three patients had anaplastic thyroid cancer.
In the present case, only high circulating levels of GM-CSF were detected, while G-CSF, TNF-α, IL-3, IL-5 levels were within the normal range. The above cytokines were measured, because they have been shown to possess eosinophilopoietic properties.28 We were unable to prove whether or not GM-CSF was produced by the tumor because immunohistochemical staining for GM-CSF could not be performed in paraffin-embedded tissue sections. We can only assume that GM-CSF was producted because of its high circulating levels and the presence of neutrophilia and eosinophilia, without any other identifiable cause of this haematologic abnormality.
Paraneoplastic leukocytosis associated with colony-stimulating factor production is an uncommon condition of unclear clinical significance. Data from patients with lung cancer showed that tumor-related leukocytosis associated with heamatopoietic cytokine production (G-CSF, GM-CSF and IL-6) is linked to poor prognosis.29 It is suggested that in our patient tumor-related leukocytosis associated with high levels of serum GM-CSF constituted a poor prognostic index in association with other factors, such as old age, tall cell variant of papillary thyroid cancer, and distant metastases at the time of the diagnosis.30,31
In conclusion, this is the first case reported in the literature of metastatic papillary thyroid cancer associated with both neutrophilia and eosinophilia and high circulating levels of GM-CSF.
REFERENCES
1. Hardy CL, Balducci L, 1985 Hemopoietic alterations of cancer. Am J Med Sci 290: 196-205.
2. Asano S, Urabe A, Okabe T, 1977 Demonstration of granulopoietic factor(s) in the plasma of nude mice transplanted with human lung cancer and in the tumor tissue. Blood 49: 845-852.
3. Kodama T, Takada K, Kameya T, Shimosato Y, Tsuchiya R, OkabeT, 1984 Large cell carcinoma of the lung associated with marked eosinophilia. Cancer 54: 2313-2317.
4. Obara T, Ito Y, Kodama T, et al, 1985 A case of gastric carcinoma associated with excessive granulocytosis. Production of a colony-stimulating factor by the tumor. Cancer 56: 782-788.
5. Sawyers CL, Golde DW, Quan S, Nimer SD, 1992 Production of granulocyte-macrophage colony-stimulating factor in two patients with lung cancer, leukocytosis and eosinophilia. Cancer 69: 1342-1346.
6. Shijubo N, Inoue Y, Hirasawa M, et al, 1992 Granulocyte colony-stimulating factor producing large cell undifferentiated carcinoma of the lung. Intern Med 31: 277-280.
7. Kojima K, Nakashima F, Boku A, Muroishi Y, Nakanishi I, Oda Y, 2002 Clinicopathological study of involvement of granulocyte colony-stimulating factor and granulo-cyte-macrophage colony-stimulating factor in non-lymphohematopoietic malignant tumors accompanied by leukocytosis. Histol Histopathol 17: 1005-1016.
8. Slungaard A, Ascensao J, Zanjani E, Jacob HS, 1983 Pulmonary carcinoma with eosinophilia. Demonstration of a tumor-derived eosinophilopoietic factor. N Engl J Med 309: 778-781.
9. Enomoto T, Sugawa H, Inoue D, et al, 1990 Establishment of a human undifferentiated thyroid cancer cell line producing several growth factors and cytokines. Cancer 65: 1971-1979.
10. Gerharz CD, Reinicke P, Schneider EM, Schmitz M, Gabbert HE, 2001 Secretion of GM-CSF and M-CSF by human renal cell carcinomas of different histologic types. Urology 58: 821-827.
11. Saito K, Kuratomi Y, Yamamoto K, et al, 1981 Primary squamous cell carcinoma of the thyroid associated with marked leukocytosis and hypercalcemia Cancer 48: 20802083.
12. Murabe H, Akamizu T, Kubota A, Kusaka S, 1992 Anaplastic thyroid carcinoma with prominent cardiac metastasis, accompanied by a marked leukocytosis with a neutrophilia and high GM-CSF level in serum. Intern Med 31: 1107-1111.
13. Yazawa S, Toshimori H, Nakatsuru K, Katakami H, Takemura J, Matsukura S. 1995 Thyroid anaplastic carcinoma producing granulocyte colony-stimulating factor and parathyroid hormone-related peptide. Intern Med 34: 584-588.
14. Iwasa K, Noguchi M, Mori K, et al, 1995 Anaplastic thyroid carcinoma producing granulocyte colony-stimulating factor (G-CSF): report of a case. Surg Today 25: 158-160.
15. Nakada T, Sato H, Inoue F, Mizorogi F, Nagayama K, Tanaka T, 1996 The production of colony-stimulating factors by thyroid carcinoma is associated with marked neutrophilia and eosinophilia. Intern Med 35: 815-820.
16. Hoshi S, Yoshizawa A, Arioka H, Kobayashi N, Kudo K, Niino H, 2000 Anaplastic thyroid carcinoma with lung metastasis producing CA 19-9 and GM-CSF. Nihon Kokyuki Gakkai Zasshi 38: 391-397.
17. Sato T, Omura M, Saito J, et al, 2000 Neutrophilia associated with anaplastic carcinoma of the thyroid: production of macrophage colony-stimulating factor (M-CSF) and interleukin-6. Thyroid 10: 1113-1118.
18. Kobayashi H, Endo K, Nishimura K, et al, 1989 A case report of thyroid papillary cancer that manifested leukocytosis and hypercalcemia after radiotherapy in bone metastasis. Gan No Rinsho 35: 55-62.
19. Balducci L, Chapman SW, Little DD, Hardy CL, 1989 Paraneoplastic eosinophilia. Report of a case with in vitro studies of hemopoiesis. Cancer 64: 2250-2253.
20. Nagel LR 1954 Eosinophilia in cancer; report of a case. N Engl J Med 280: 607.
21. Miller WM, Adcook KJ, Moniot AL, Raymond LW, Hutcheson J, Elliot RC, 1977 Progressive hypereosinophilia with lung nodules due to thyroid carcinoma. Chest 71: 789-791.
22. Van Crombrugge P, Pauwels R, Van der Straeten M, 1983 Thyroid carcinoma and eosinophilia Ann Clin Res 15: 128-130.
23. Yoshida A, Asaga T, Masuzawa C, et al, 1994 Production of cytokines by thyroid carcinoma cell lines. J Surg Oncol 55: 104-107.
24. Asakawa H, Kobayashi T, 1999 The secretion of cytokines and granulocyte colony stimulating factor by anaplastic and poorly differentiated thyroid carcinoma cell lines Anticancer Res 19: 761-764.
25. Aust G, Hofmann A, Laue S, Ode-Hakim S, Scherbaum WA, 1996 Differential regulation of granulocyte-macrophage colony-stimulating factor mRNA and protein expression in human thyrocytes and thyroid-derived fi-broblasts by interleukin-1 and tumour necrosis factor-. J Endocrinol 151: 277-285.
26. Kasai K, Banba N, Motohashi S, et al, 1997 Production of granulocyte/macrophage and macrophage colony-stimulating factor by human thyrocytes in culture. Biochem Biophys Res Commun 238: 191-196.
27. Russell JP, Engiles JB, Rothstein JL, 2004 Proinflammatory mediators and genetic background in oncogene mediated tumor progression. J Immunol 172: 4059-4067.
28. Devereux S, Linch DC 1998 Granulocyte-macrophage colony-stimulating factor. In: Mire-Sluis A, Thorpe R (eds), Cytokines, London, Academic; p, 261-275.
29. Kasuga I, Makino S, Kiyokawa H, Katoh H, Ebihara Y, Ohyashiki K, 2001 Tumor-related leukocytosis is linked with poor prognosis in patients with lung carcinoma. Cancer 92: 2399-405.
30. Schlumberger M, Pacini F 2003 Prognostic factors. In: Thyroid tumors, Nucleon Editions, Paris; pp, 111-125.
31. Tzavara I, Vlassopoulou B, Alevizaki C, Koukoulis G, Tzanela M, Koumoussi P, Sotsiou F, Thalassinos N, 1999 Differentiated thyroid cancer: a retrospective analysis of 832 cases from Greece Clin Endocrinol (Oxf) 50: 643-654.