Abstract
–
INTRODUCTION
Cushings’s syndrome due to ectopic adrenocorticotrophin (ACTH) secretion was first described nearly a century ago by Hurst Brown.1 Bronchial carcinomas, usually bronchial carcinoids, were the first to be described and continue to be the leading cause of the ectopic ACTH syndrome; however, thymic carcinoids account for approximately 10% of cases.2 The Zollinger Ellison syndrome, excessive gastrin secretion from a neuroendcorine tumour, has been described as exclusively due to neuroendocrine tumours of entero-pancreatic origin, while secretion of gastrin from a thymic carcinoid tumour has not been reported to our knowledge. We report a unique case of a 34-year-old woman with ACTH-dependent Cushing’s syndrome and Zollinger-Ellison syndrome due to a thymic carcinoid tumour.
CASE REPORT
A 34-year-old woman, diagnosed with diabetes mellitus 8 months previously, presented with poor blood glucose control requiring frequent escalations of her insulin dose. In addition, she had epigastric pain with frequent episodes of melaena which failed to respond to proton pump inhibitors (PPI) at standard doses. She also had progressive pigmentation of the body, amenorrhoea, increased growth of facial hair, acne and proximal muscle weakness. Several months prior to this presentation she had also noticed weight loss and lower back pain.
Physical examination revealed signs of Cushing’s syndrome including thinning of the skin resulting in bruises over the forearms, purple striae in the abdomen, acne, hirsutism, diffuse pigmentation of the skin, proximal myopathy and a raised blood pressure (160/100 mmHg). She also had marked tenderness over the epigastric area of her abdomen and in her lower back over the thoraco-lumbar spine.
Routine biochemistry revealed elevated blood glucose levels (>200 mg/dl) and hypokalaemic alkalosis (K+3 mmol/L, HCO3ˉ 32 mmol/L). Serum creatinine phosphokinase, blood urea, calcium and thyroid function tests were within the normal range. The results of special endocrine tests for Cushing’s syndrome are shown in Table 1.
The chronic epigastric pain was investigated with upper gastrointestinal endoscopy which showed pan-gastritis with increased mucosal rugosity. Gastric mucosal biopsy of the gastric fundus showed cystic dilatation of the glands and hyperplasia of the secretory portions with an increased number of parietal cells. This appearance was consistent with the Zollinger-Ellison syndrome. A fasting gastrin level (off PPI for one month) was grossly elevated at 542 pg/ml (normal range 13–15 pg/ml; the gastrin levels were measured using the Immulite/Immulite 1000 ELCLA); 24 hr urinary 5HIAA excretion and plasma chromogranin A levels were normal.
Computed tomographic (CT) scanning of the abdomen showed bilateral adrenal hyperplasia. The stomach wall appeared thickened with prominent rugae. The pancreas was normal (Figure 1). Magnetic resonance imaging (MRI) of the pituitary was normal. However, CT scanning of the thorax revealed a large mass suggestive of a thymic tumour (Figure 2).
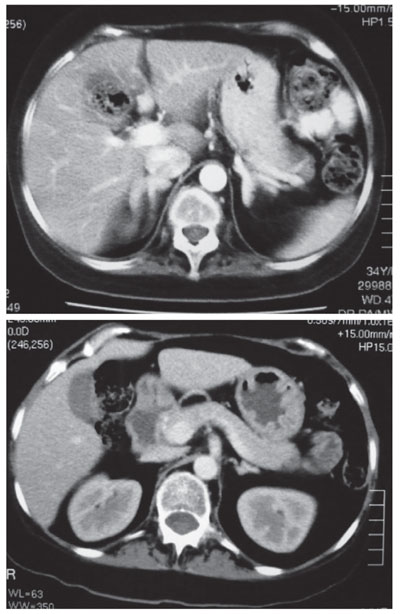
Figure 1. Computed Tomographic scans show bilateral adrenal hyperplasia and thickened gastric wall with prominent rugae.
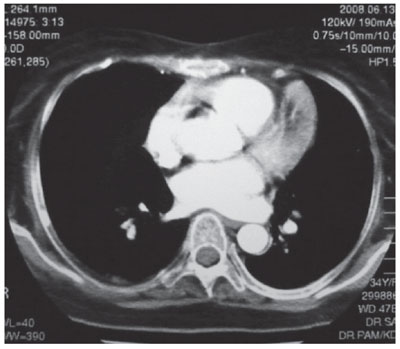
Figure 2. CT thorax showing thymic tumour.
Based on the biochemical and imaging findings, the possibility of a thymic neuroendocrine tumour (‘carcinoid’) secreting both gastrin and ACTH was considered. However, a second tumour in the pancreas or duodenum secreting gastrin required exclusion. Preoperative localization of gastrinomas by current imaging techniques such as CT scanning and angiography is still difficult because of the small size of tumour(s) in most patients undergoing evaluation.3 We therefore planned venous sampling for gastrin from a series of sites to establish the source of the elevated gastrin.
A catheter study was planned to sample venous blood from sites draining from the entero-pancreatic circulation and from thymic veins. Sampling of the entero-pancreatic system involves a transhepatic approach to enter into the portal venous system. We planned to sample hepatic and thymic veins first and then proceed to the transhepatic sampling only if initial results were inconclusive. A venous catheter was advanced from the right femoral vein through the inferior vena cava, hepatic veins and right brachiocephalic vein to the left brachiocephalic vein, which directly drains the thymus. Blood samples were drawn from each site for gastrin and ACTH (Table 2). The highest gastrin and ACTH levels were found in the left brachiocephalic vein compared to the other sites, although the gradient was not massive. The relatively lower levels seen in the hepatic veins rendered the possibility of a duodenal or pancreatic site less likely. These results suggested that the thymic tumour was indeed the source of excess gastrin and ACTH.
The patient was then prepared for thymectomy. The general medical condition of the patient needed to be optimised prior to surgery. Therefore, her Cushing’s was first treated medically with ketoconazole and the response to treatment was assessed by mean cortisol levels derived from cortisol ‘day-curves’. Her hypokalaemia, blood glucose and myopathy improved with ketoconazole, and she subsequently underwent thymectomy. The surgeons were able to identify the thymic vein (Figure 3), which was then cannulated and blood samples taken for ACTH and gastrin levels. A marked but incomplete fall in both hormones was evident immediately following the removal of the tumour (Table 3), suggesting that the thymic tumour was responsible for both gastrin and ACTH, and also that resection was not complete.
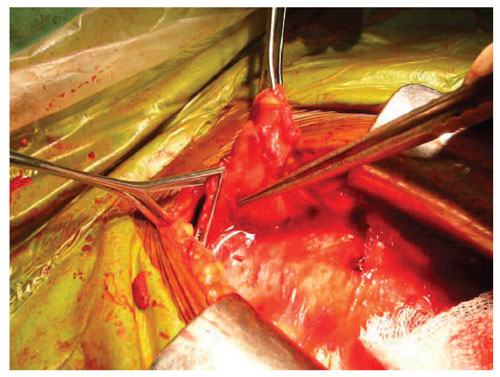
Figure 3. The thymic vein was identified and cannulated during surgery.
Following the surgery, the patient improved dramatically and her blood glucose normalised within a short period. There was a marked improvement in hypertension, proximal myopathy and epigastric pain. She was able to carry out her normal daily activities with only some limitations caused by persistent backache due to osteoporosis. However, her gastrin and ACTH failed to return to normal levels and external beam radiotherapy was planned as the next strategy.
The histology demonstrated a thymic neuroendocrine tumour with positive immunostaining for both gastrin and ACTH.
DISCUSSION
The diagnosis of the ectopic ACTH syndrome was suspected in this patient due to presence of florid features of Cushing’s syndrome such as pigmentation, hypokalaemia, difficult-to-control diabetes requiring high-dose insulin and marked proximal myopathy. This was also strongly suggested by high levels of ACTH and failure to suppress cortisol with high-dose dexamethasone. MRI scanning of the pituitary was negative. The pre-test probability of a woman with ACTH-dependent Cushing’s syndrome having a lesion in the pituitary is in the region of 90%;4 however, this patient’s clinical presentation was more characteristic of ectopic ACTH, this diagnosis being supported by the short duration and aggressive progression of symptoms.
Though bronchial carcinoids and small cell carcinomas of the lung are recognised as the commonest cause of the ectopic ACTH syndrome, there is accumulating evidence that thymic carcinoids are also responsible for many cases.2 Multiple endocrine neoplasia type 1 (MEN 1), a syndrome with an autosomal dominant pattern of inheritance, manifests with development of tumours in three principal glands, namely the parathyroids, the anterior pituitary and the endocrine pancreas. It has been reported that thymic carcinoids are very common (85%) in patients with MEN 1,5 and this association has practically always been seen in male smokers.6 However, while the ectopic ACTH syndrome due to a thymic carcinoid is rare in MEN 1, it has been described.7 Our patient did not have a positive family history for MEN 1, and the fact that her calcium was repeatedly normal excluded primary hyperparathyroidism, an almost invariable finding in MEN 1.
Zollinger-Ellison syndrome, on the other hand, is almost always due to tumours of entero-pancreatic origin. Despite long-term PPI treatment, gastrointestinal endoscopy in this patient revealed pan-gastritis. Hypertrophic gastric rugae were a notable finding and the histological feature of parietal cell hyperplasia and changes in glandular epithelium were consistent with that of the Zollinger-Ellison syndrome. As chronic PPI ingestion can result in hypergastrinaemia, we allowed a sufficient PPI-free period before checking the fasting gastrin level to permit the effect of drugs to wear off. Although we did not perform gastric acid secretory or other provocative tests, the typical gastric histology with a greatly raised gastrin level in the thymic veins suggest that the Zollinger-Ellison syndrome, a gastrinoma, is the most likely diagnosis here.
Thus, the possibility of having two tumours was entertained. Endoscopic ultrasonography is considered as a first-choice imaging technique for the preoperative detection of gastrinomas. Although small duodenal gastrinomas are difficult to detect, an accurate exploration of the pancreatic area is provided by this technique.3 However, since this technique was not available at our centre, a venous catheter study was performed instead.
Co-secretion of gastrin along with ACTH from the thymic carcinoid tissue in this patient is supported by three different techniques: firstly, she had the highest concentration of gastrin in the veins draining the thymus; secondly, she showed a rapid albeit partial fall in gastrin immediately following thymectomy; and finally, the immunofluoresence techniques demonstrating gastrin positivity in the thymic tissue provided conclusive proof that the Zollinger-Ellison syndrome in this patient was due to a thymic carcinoid tumour co-secreting gastrin and ACTH.
CONCLUSIONS
To our knowledge, there has been no reported case of a thymic carcinoid secreting both ACTH and gastrin.7 This case illustrates the pluri-potential nature of neuroendocrine tumours in their hormone-secretory capability. Furthermore, the thymus may be an ectopic source of gastrin producing the Zollinger-Ellison syndrome and this should be borne in mind when investigations and treatment strategies are planned in such patients.
REFERENCES
1.Brown WH, 1928 A case of pluriglandular syndrome: “diabetes of bearded women”. Lancet 212: 1022-1023.
2.Beuschlein F, Hammar GD, 2002 Ectopic pro-opiomelanocortin syndrome. End Met Clin Noth Am 31: 191-234.
3.Ruszniewski P, Amouyal P, Amouyal G, et al, 1995 Localization of gastrinomas by endoscopic ultrasonography in patients with Zollinger-Ellison syndrome. Surgery 117: 629-635.
4.Newell-Price J, Bertagna X, Grossman AB, Nieman LK, 2006 Cushing’s syndrome, Lancet 367: 1605-1617.
5.Gibril F, Chen YJ, Schrump DS, et al, 2003 Prospective Study of Thymic Carcinoids in Patients with Multiple Endocrine Neoplasia Type 1. J Clin Endocrinol Metab 88: 1066-1081.
6.Ferolla P, Falchetti A, Filosso P, et al, 2005 Thymic Neuroendocrine Carcinoma (Carcinoid) in Multiple Endocrine Neoplasia Type 1 Syndrome: The Italian Series. J Clin Endocrinol Metab 90: 2603-2609.
7.Ghazi AA, Dezfooli AA, Mohamadi F, et al, 2011 Cushing’s syndrome secondary to a thymic carcinoid tumor due to multiple endocrine neoplasia type 1. Endocr Pract, 17: e92-6.
8.Kaltsas G, Androulakis II, de Herder WW, Grossman AB, 2010 Paraneoplastic syndromes and neuroendocrine tumours. Endocr Relat Cancer 17: R173-R193.
Address for correspondence:
Dr. N. Somasundaram, The National Hospital of Sri Lanka,
Colombo 10, Sri Lanka, Tel.: 0094773660923,
e-mail: noelsomasundaram@gmail.com
Received 20-08-2012, Accepted 31-10-2012